

Signaling Through FcγRIIA and the C5a-C5aR Pathway Mediate Platelet Hyperactivation in COVID-19
- PMID: 35309299
- PMCID: PMC8928747
- DOI: 10.3389/fimmu.2022.834988
Signaling Through FcγRIIA and the C5a-C5aR Pathway Mediate Platelet Hyperactivation in COVID-19
Abstract
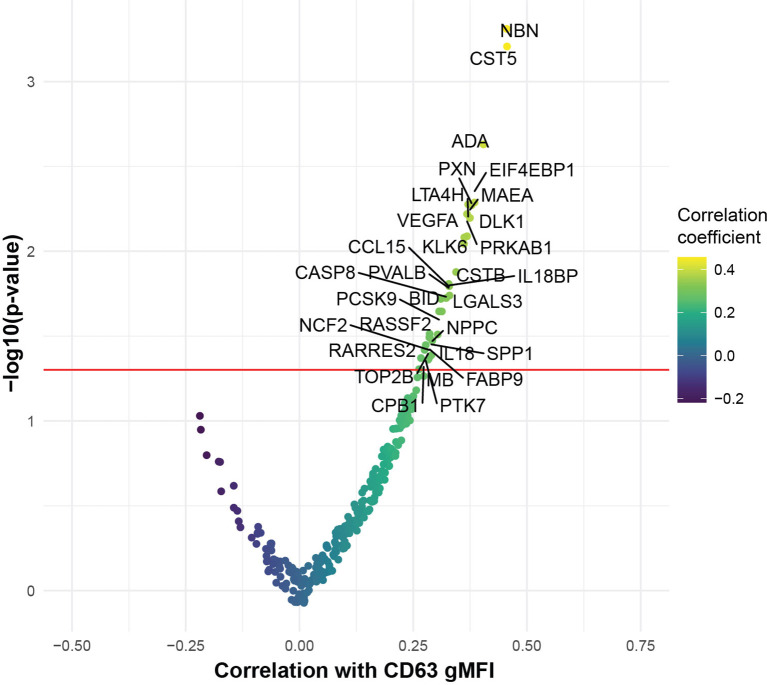
Patients with COVID-19 present with a wide variety of clinical manifestations. Thromboembolic events constitute a significant cause of morbidity and mortality in patients infected with SARS-CoV-2. Severe COVID-19 has been associated with hyperinflammation and pre-existing cardiovascular disease. Platelets are important mediators and sensors of inflammation and are directly affected by cardiovascular stressors. In this report, we found that platelets from severely ill, hospitalized COVID-19 patients exhibited higher basal levels of activation measured by P-selectin surface expression and had poor functional reserve upon in vitro stimulation. To investigate this question in more detail, we developed an assay to assess the capacity of plasma from COVID-19 patients to activate platelets from healthy donors. Platelet activation was a common feature of plasma from COVID-19 patients and correlated with key measures of clinical outcome including kidney and liver injury, and APACHEIII scores. Further, we identified ferritin as a pivotal clinical marker associated with platelet hyperactivation. The COVID-19 plasma-mediated effect on control platelets was highest for patients that subsequently developed inpatient thrombotic events. Proteomic analysis of plasma from COVID-19 patients identified key mediators of inflammation and cardiovascular disease that positively correlated with in vitro platelet activation. Mechanistically, blocking the signaling of the FcγRIIa-Syk and C5a-C5aR pathways on platelets, using antibody-mediated neutralization, IgG depletion or the Syk inhibitor fostamatinib, reversed this hyperactivity driven by COVID-19 plasma and prevented platelet aggregation in endothelial microfluidic chamber conditions. These data identified these potentially actionable pathways as central for platelet activation and/or vascular complications and clinical outcomes in COVID-19 patients. In conclusion, we reveal a key role of platelet-mediated immunothrombosis in COVID-19 and identify distinct, clinically relevant, targetable signaling pathways that mediate this effect.
Keywords: COVID - 19; FcγRIIa; complement; fostamatinib; platelet.
Copyright © 2022 Apostolidis, Sarkar, Giannini, Goel, Mathew, Suzuki, Baxter, Greenplate, Alanio, Abdel-Hakeem, Oldridge, Giles, Wu, Chen, Huang, Belman, Pattekar, Manne, Kuthuru, Dougherty, Weiderhold, Weisman, Ittner, Gouma, Dunbar, Frank, Huang, Vella, The UPenn COVID Processing Unit, Reilly, Hensley, Rauova, Zhao, Meyer, Poncz, Abrams and Wherry.
Conflict of interest statement
SH has received consultancy fees from Sanofi Pasteur, Lumen, Novavax, and Merck for work unrelated to this report. AH is a consultant for Immunai. EW is consulting or is an advisor for Merck, Elstar, Janssen, Related Sciences, Synthekine and Surface Oncology. EW is a founder of Surface Oncology and Arsenal Biosciences. EW is an inventor on a patent (US Patent number 10,370,446) submitted by Emory University that covers the use of PD-1 blockade to treat infections and cancer. NM reports funding to her institution from Quantum Leap Healthcare Collaborative, Athersys, Inc., Biomarck, Inc. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Update of
-
Signaling through FcγRIIA and the C5a-C5aR pathway mediates platelet hyperactivation in COVID-19.bioRxiv [Preprint]. 2021 May 3:2021.05.01.442279. doi: 10.1101/2021.05.01.442279. bioRxiv. 2021. Update in: Front Immunol. 2022 Mar 03;13:834988. doi: 10.3389/fimmu.2022.834988. PMID: 33972943 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
- R38 HL143613/HL/NHLBI NIH HHS/United States
- K08 CA230157/CA/NCI NIH HHS/United States
- R01 HL137006/HL/NHLBI NIH HHS/United States
- T32 HL007586/HL/NHLBI NIH HHS/United States
- T32 CA009140/CA/NCI NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- T32 HL007775/HL/NHLBI NIH HHS/United States
- P01 HL040387/HL/NHLBI NIH HHS/United States
- R35 HL150698/HL/NHLBI NIH HHS/United States
- P01 HL120846/HL/NHLBI NIH HHS/United States
- F99 CA234842/CA/NCI NIH HHS/United States
- R01 HL137915/HL/NHLBI NIH HHS/United States
- UM1 AI069534/AI/NIAID NIH HHS/United States
- K08 AI136660/AI/NIAID NIH HHS/United States
- R01 AI105343/AI/NIAID NIH HHS/United States
- T32 AR076951/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous