

Benign Recurrent Vertigo: The Course of Vertigo Attacks Compared to Patients With Menière's Disease and Vestibular Migraine
- PMID: 35309556
- PMCID: PMC8924118
- DOI: 10.3389/fneur.2022.817812
Benign Recurrent Vertigo: The Course of Vertigo Attacks Compared to Patients With Menière's Disease and Vestibular Migraine
Abstract
Objective: To explore the course of vertigo attacks in patients with benign recurrent vertigo (BRV) as compared to patients with Menière's disease (MD) and vestibular migraine (VM).
Study design: Prospective cohort study.
Setting: Tertiary referral center.
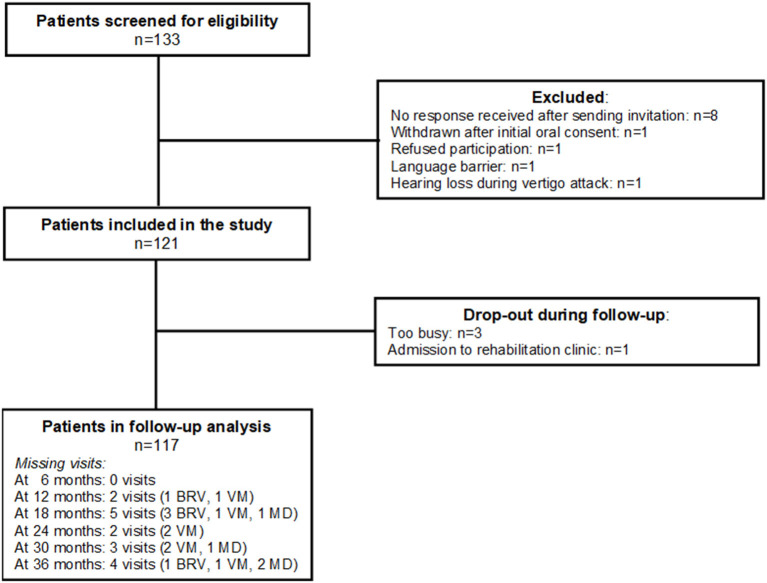
Patients: Adult patients who visited the Apeldoorn Dizziness Center between January 2015 and November 2016 and who were diagnosed with BRV, VM or MD. During 3 years participants were contacted every 6 months by telephone to complete a study-specific questionnaire.
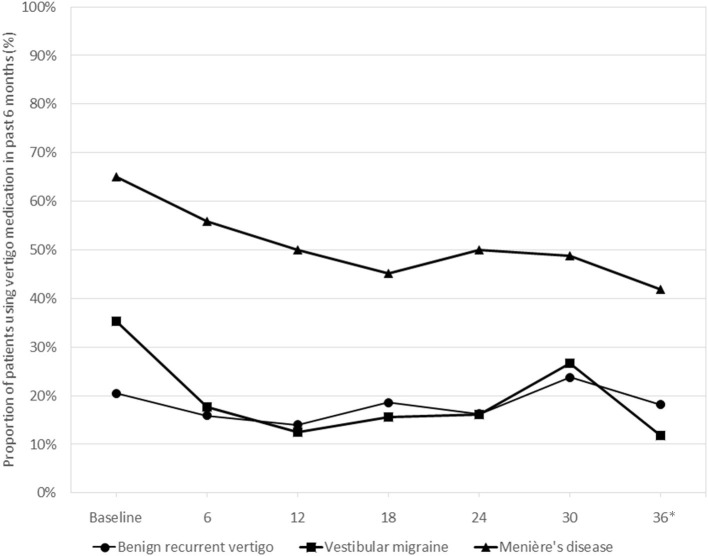
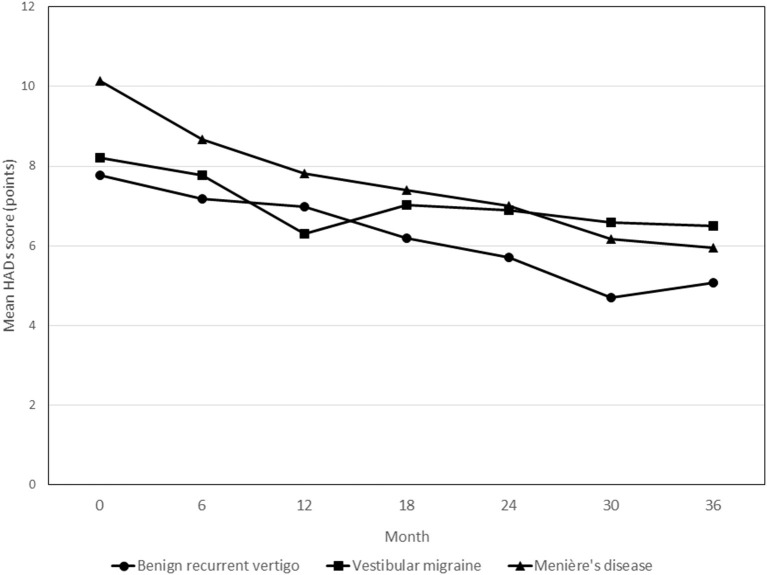
Main outcome measures: Vertigo attack frequency, use of medication, and Hospital Anxiety and Depression Scale (HADS).
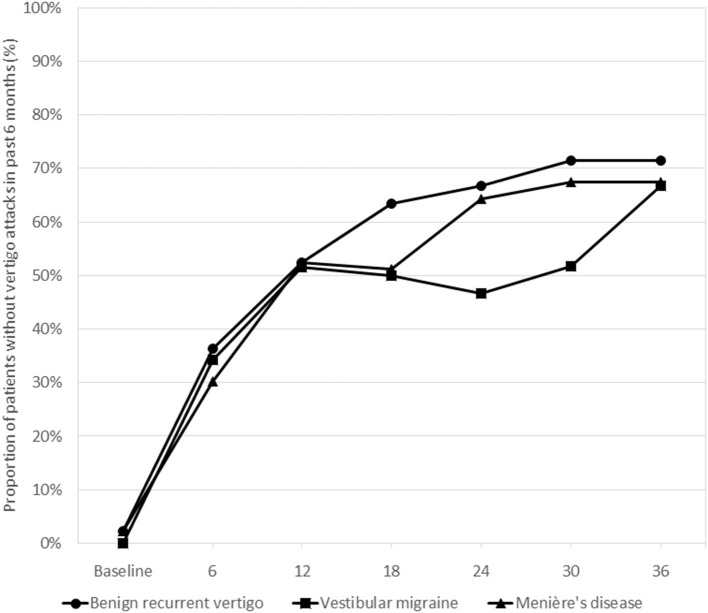
Results: The study population (n = 121) consisted of 44 patients with BRV, 34 with VM, and 43 with MD. For the total follow-up period no statistically significant differences between the three diagnosis groups were observed for being attack-free in the past 6 months: OR = 0.86 (95% CI 0.34-2.17; p = 0.745) for VM and OR = 1.06 (95% CI 0.44-2.51; p = 0.902) for MD, compared to BRV. Overall, 19 patients (43.2%) with BRV, 13 (38.2%) with VM, and 35 (81.0%) with MD used medication to prevent vertigo attacks at any point during their 3-year follow-up. Throughout the observation period patients with MD showed an average of 3.37 points (95% CI 0.68-6.07; p = 0.014) higher HADS scores relative to patients with BRV.
Conclusion: The course of vertigo attacks was rather favorable in the three groups, as 67-70% of the patients were free of vertigo attacks after 3 years of follow-up. The course of disease in patients with BRV was not distinctive from patients with MD and VM. We assume that BRV is a mild or incomplete variant of VM and MD, rather than a separate disease entity with distinct pathognomonic features.
Keywords: Menière's disease; attacks; benign recurrent vertigo; medication; mental health limitations; prognosis; vestibular migraine.
Copyright © 2022 van Leeuwen, Colijn, van Esch and Schermer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous