

Labyrinthine Fistula in Cholesteatoma Patients: Outcomes of Partial Labyrinthectomy With "Underwater Technique" to Preserve Hearing
- PMID: 35309574
- PMCID: PMC8924537
- DOI: 10.3389/fneur.2022.804915
Labyrinthine Fistula in Cholesteatoma Patients: Outcomes of Partial Labyrinthectomy With "Underwater Technique" to Preserve Hearing
Abstract
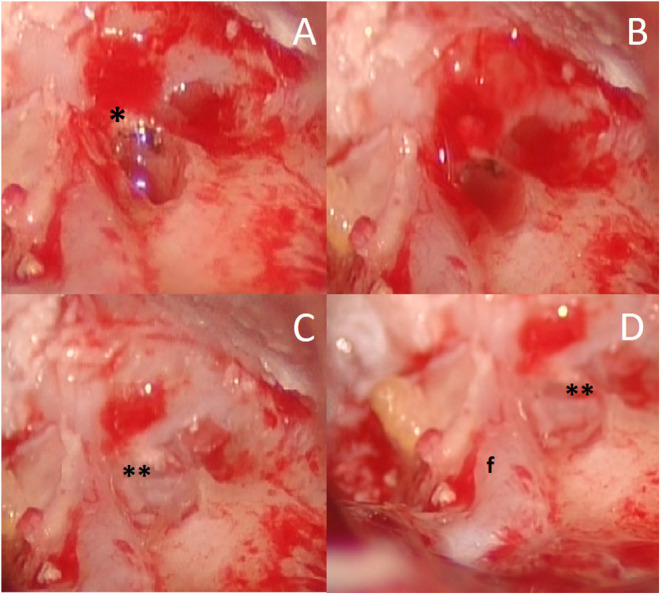
Labyrinthine fistula (LF) is one of the most important complications of cholesteatoma and is defined as an abnormal communication between the inner and the middle ear. This study aims to describe our experience with the partial labyrinthectomy evaluating the post-operative hearing results. Twenty-one patients who presented labyrinthine fistula in the semicircular canals were included in the present study. Hearing impairment was present in 48% of patients (10/21). A pre-operative assessment using the Gardner-Robertson hearing classification showed the following: 52%, Class I; and 48%, Class II. A post-surgical Gardner-Robertson hearing classification evidenced the following: 43%, Class I; and 57%, Class II. The presence of LF is usually considered a negative prognostic factor for hearing preservation. The key point of partial labyrinthectomy surgery is the preservation of structures, keeping them wet with Ringer's solution throughout the procedures, and not performing suction that is close to the opened LF. The bony labyrinth is drilled underwater without suction, removing the entire cholesteatoma matrix and quickly plugging the site before and after the LF. This faster plugging of the labyrinth makes it possible to preserve the peri-lymph and the endo-lymph fluid and the hearing function. This study showed that a partial labyrinthectomy is useful for maintaining serviceable hearing in patients with LF.
Keywords: cholesteatoma; fistula; labyrinth diseases; otologic surgical procedure; underwater technique.
Copyright © 2022 Pace, Milani, Messineo, Rossetti, Cocuzza, Maniaci, Vicini, Iannella and Magliulo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Endoscopic diving technique for hearing preservation in managing labyrinth-invading cholesteatomas.Eur Arch Otorhinolaryngol. 2023 Apr;280(4):1639-1646. doi: 10.1007/s00405-022-07635-w. Epub 2022 Sep 7. Eur Arch Otorhinolaryngol. 2023. PMID: 36071251
-
Clinical Study of Labyrinthine Fistula in Cholesteatomatous Chronic Otitis Media: A Tertiary Care Hospital-Based Retrospective Study in a South Indian Population.Cureus. 2023 Jul 25;15(7):e42413. doi: 10.7759/cureus.42413. eCollection 2023 Jul. Cureus. 2023. PMID: 37637549 Free PMC article.
-
[A case of hearing preservation during surgical treatment of distributed fistula labyrinth in a patient with chronic purulent means otitis and cholesteatoma].Vestn Otorinolaringol. 2022;87(3):99-106. doi: 10.17116/otorino20228703199. Vestn Otorinolaringol. 2022. PMID: 35818953 Review. Russian.
-
Lateral semicircular canal fistula in cholesteatoma: diagnosis and management.Eur Arch Otorhinolaryngol. 2016 Aug;273(8):2055-63. doi: 10.1007/s00405-015-3775-6. Epub 2015 Sep 8. Eur Arch Otorhinolaryngol. 2016. PMID: 26351038
-
Hearing and vertigo outcomes after congenital labyrinthine cholesteatoma resection.Am J Otolaryngol. 2014 May-Jun;35(3):417-23. doi: 10.1016/j.amjoto.2014.01.004. Epub 2014 Jan 10. Am J Otolaryngol. 2014. PMID: 24503247 Review.
Cited by
-
Development of semicircular canal occlusion.Front Neurosci. 2022 Aug 19;16:977323. doi: 10.3389/fnins.2022.977323. eCollection 2022. Front Neurosci. 2022. PMID: 36061608 Free PMC article.
References
-
- Romanet P., Duvillard C, Delouane M, Vigne P, De Raignac E, Darantiere S, et al. . Labyrinthine fistulae and cholesteatoma. Ann Otolaryngol Chir Cervicofac. (2001) 118:181–6. - PubMed
LinkOut - more resources
Full Text Sources