

Care transitions intervention reduces ED revisits in cognitively impaired patients
- PMID: 35310533
- PMCID: PMC8919246
- DOI: 10.1002/trc2.12261
Care transitions intervention reduces ED revisits in cognitively impaired patients
Abstract
Introduction: About half of older adults with impaired cognition who are discharged home from the emergency department (ED) return for further care within 30 days. We tested the effect of an adapted Care Transitions Intervention (CTI) at reducing ED revisits in this vulnerable population.
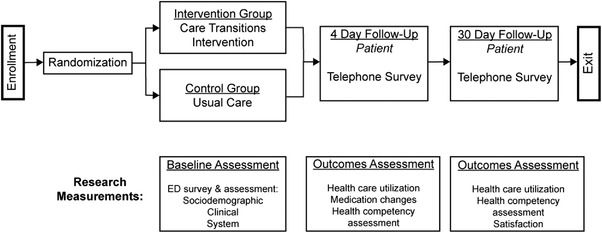
Methods: We conducted a pre-planned subgroup analysis of community-dwelling, cognitively impaired older (age ≥60 years) participants from a randomized controlled trial testing the effectiveness of the CTI adapted for ED-to-home transitions. The parent study recruited ED patients from three university-affiliated hospitals from 2016 to 2019. Subjects eligible for this sub-analysis had to: (1) have a primary care provider within these health systems; (2) be discharged to a community residence; (3) not receive care management or hospice services; and (4) be cognitively impaired in the ED, as determined by a score >10 on the Blessed Orientation Memory Concentration Test. The primary outcome, ED revisits within 30 days of discharge, was abstracted from medical records and evaluated using logistic regression.
Results: Of our sub-sample (N = 81, 36 control, 45 treatment), 57% were female and the mean age was 78 years. Multivariate analysis, adjusted for the presence of moderate to severe depression and inadequate health literacy, found that the CTI significantly reduced the odds of a repeat ED visit within 30 days (odds ratio [OR] 0.25, 95% confidence interval [CI] 0.07 to 0.90) but not 14 days (OR 1.01, 95% CI 0.26 to 3.93). Multivariate analysis of outpatient follow-up found no significant effects.
Discussion: Community-dwelling older adults with cognitive impairment receiving the CTI following ED discharge experienced fewer ED revisits within 30 days compared to usual care. Further studies must confirm and expand upon this finding, identifying features with greatest benefit to patients and caregivers.
Keywords: care transitions; care transitions intervention; cognitive impairment; community paramedicine; dementia; emergency; emergency department.
© 2022 The Authors. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring published by Wiley Periodicals, LLC on behalf of Alzheimer's Association.
Conflict of interest statement
MNS–Research reported in this publication received support from the National Institute on Aging of the National Institutes of Health under Award Number R01AG050504 and K24AG054560 and the Clinical and Translational Science Award program, through the NIH National Center for Advancing Translational Sciences award UL1TR002373. Grants have been received from NIH, and payments were made to my institution. Contracts have been received from Omron and Lumos, and payments were made to my institution. In the past 36 months, received consulting fees from the University of Cincinnati, University of Colorado, University at Buffalo, NIH, American Federation for Aging Research, Geriatric ED Collaborative, and Mt. Sinai School of Medicine. In the past 36 months, I received support for attending meetings and/or travel for/to the following: American College of Emergency Physicians, American Federation for Aging Research, American Geriatrics Society, NIH, Society for Academic Emergency Medicine, University at Buffalo, University of Cincinnati, and University of Colorado. In the past 36 months, I participated on a Data Safety Monitoring Board/Advisory Board for the NIH and payments were made to me. In the past 36 months, I held leadership position in the Society for Academic Emergency Medicine Foundation (received no payments) and the Isthmus Project (received no payments).
Figures
References
-
- Pitts SR, Carrier ER, Rich EC, Kellerman AL. Where Americans get acute care: increasingly it's not at their doctor's office. Health Affairs (Millwood). 2010;29:1620‐1629. - PubMed
-
- Trends in Emergency Department Visits ‐ HCUP Fast Stats. Retrieved December 3, 2020, from https://www.hcup‐us.ahrq.gov/faststats/NationalTrendsEDServlet?measure1=...
-
- McCusker J, Cardin S, Bellavance F, et al. Return to the emergency department among elders: patterns and predictors. Acad Emerg Med Off J Soc Acad Emerg Med. 2000;7(3):249‐259. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources