

Determinants of SARS-CoV-2 transmission to guide vaccination strategy in an urban area
- PMID: 35310621
- PMCID: PMC8927799
- DOI: 10.1093/ve/veac002
Determinants of SARS-CoV-2 transmission to guide vaccination strategy in an urban area
Abstract
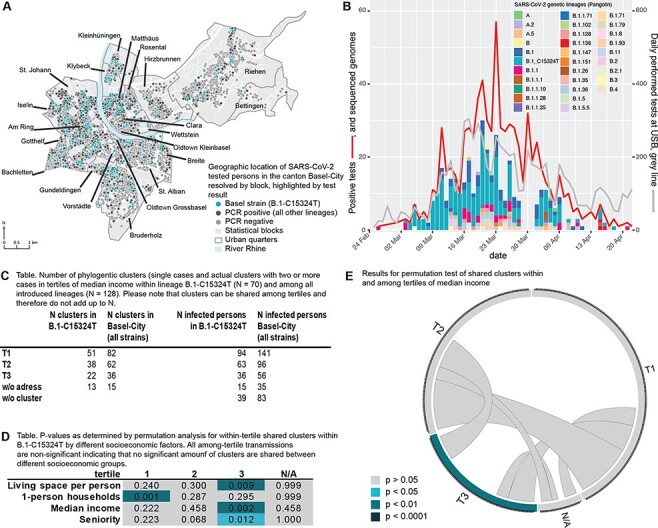
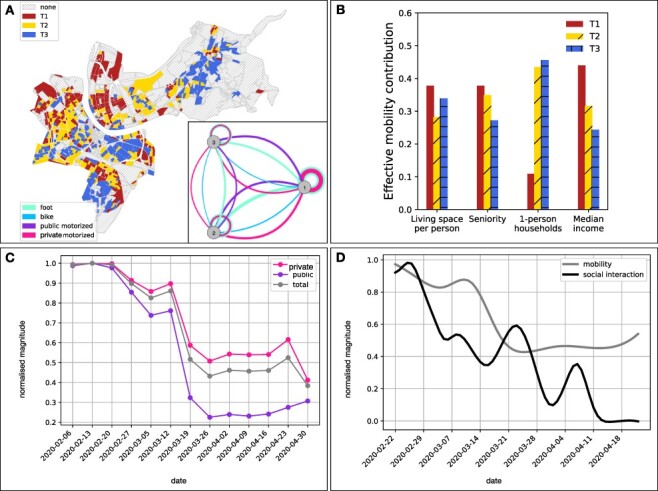
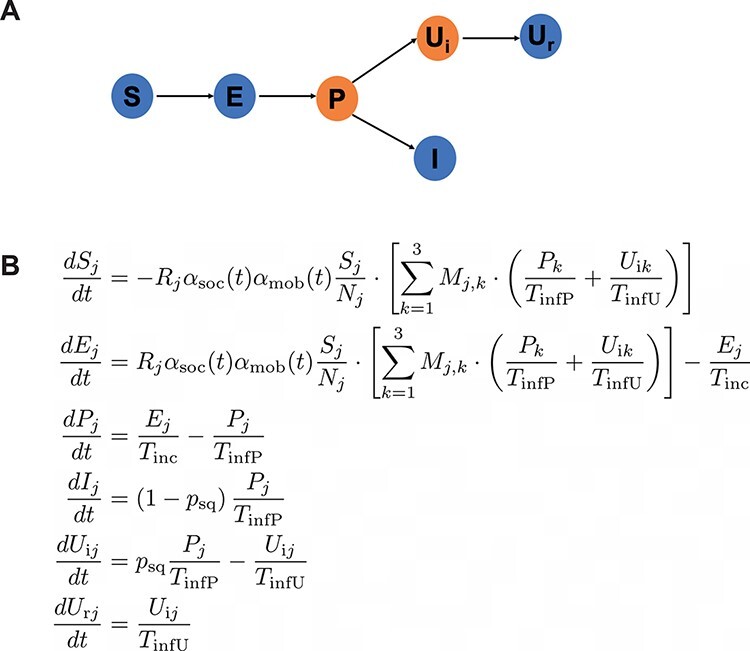
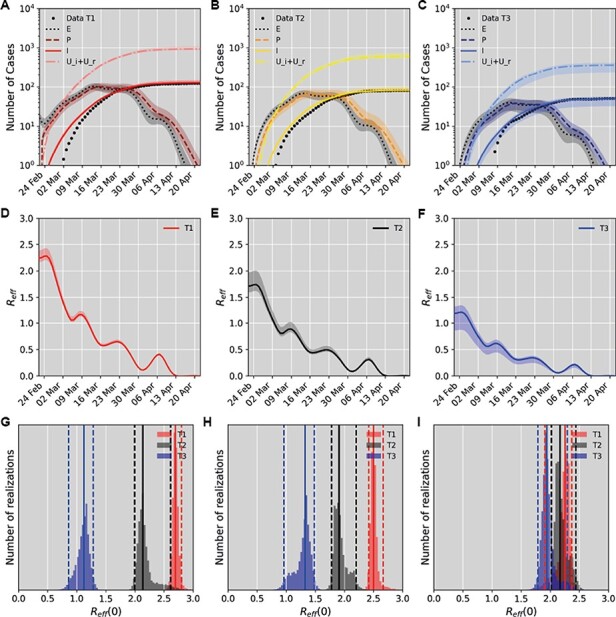
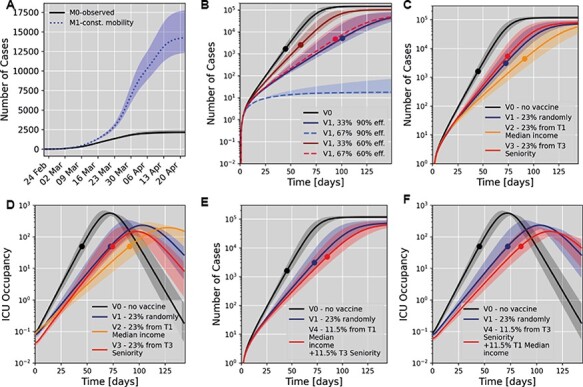
Transmission chains within small urban areas (accommodating ∼30 per cent of the European population) greatly contribute to case burden and economic impact during the ongoing coronavirus pandemic and should be a focus for preventive measures to achieve containment. Here, at very high spatio-temporal resolution, we analysed determinants of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission in a European urban area, Basel-City (Switzerland). We combined detailed epidemiological, intra-city mobility and socio-economic data sets with whole-genome sequencing during the first SARS-CoV-2 wave. For this, we succeeded in sequencing 44 per cent of all reported cases from Basel-City and performed phylogenetic clustering and compartmental modelling based on the dominating viral variant (B.1-C15324T; 60 per cent of cases) to identify drivers and patterns of transmission. Based on these results we simulated vaccination scenarios and corresponding healthcare system burden (intensive care unit (ICU) occupancy). Transmissions were driven by socio-economically weaker and highly mobile population groups with mostly cryptic transmissions which lacked genetic and identifiable epidemiological links. Amongst more senior population transmission was clustered. Simulated vaccination scenarios assuming 60-90 per cent transmission reduction and 70-90 per cent reduction of severe cases showed that prioritising mobile, socio-economically weaker populations for vaccination would effectively reduce case numbers. However, long-term ICU occupation would also be effectively reduced if senior population groups were prioritised, provided there were no changes in testing and prevention strategies. Reducing SARS-CoV-2 transmission through vaccination strongly depends on the efficacy of the deployed vaccine. A combined strategy of protecting risk groups by extensive testing coupled with vaccination of the drivers of transmission (i.e. highly mobile groups) would be most effective at reducing the spread of SARS-CoV-2 within an urban area.
© The Author(s) 2022. Published by Oxford University Press.
Figures
References
-
- AstraZeneca (2020), ‘AZD1222 vaccine met primary efficacy endpoint in preventing COVID-19’.
-
- Bau- und Verkehrsdepartement Basel-Stadt Mobilität / Mobilitätsstrategie (2020), ‘Gesamtverkehrsmodell der Region Basel, Basismodell: “Ist-Zustand 2016”’.
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
