

Serrated polyposis syndrome with multiple inverted lesions in the colon: Case report and elucidation of morphogenetic mechanism
- PMID: 35310715
- PMCID: PMC8828188
- DOI: 10.1002/deo2.13
Serrated polyposis syndrome with multiple inverted lesions in the colon: Case report and elucidation of morphogenetic mechanism
Abstract
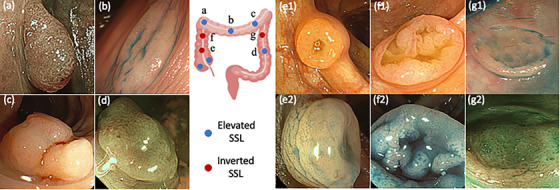
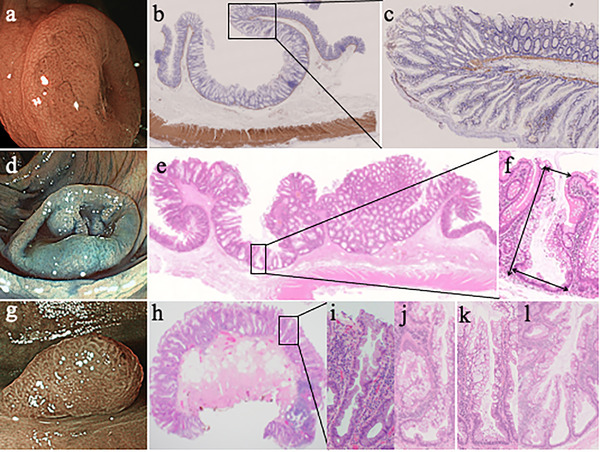
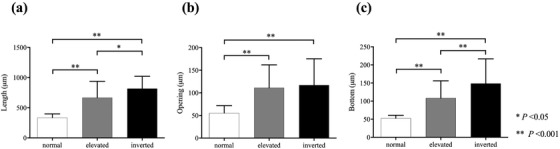
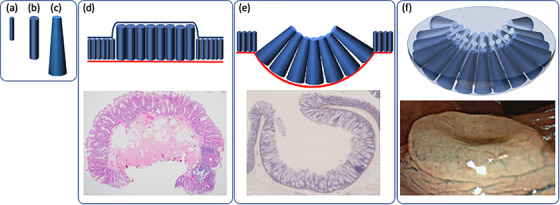
A 70-year-old man underwent surveillance colonoscopy following surgery for occlusive sigmoid colon cancer. The procedure revealed nine sessile serrated lesions (SSLs), including three inverted lesions. Endoscopic and surgical resections were performed. All nine lesions were confirmed pathologically as SSL, and the patient was diagnosed with serrated polyposis syndrome (SPS). Three inverted SSLs (iSSLs) showed endophytic growth without epithelial misplacement. Crypt analysis revealed that iSSL crypts were wider at the bottom than the opening, roughly resembling a frustoconical shape. Our results suggest that a horizontal arrangement of frustoconical crypts leads to hemispherical deformation of the muscularis mucosa, forming an inverted shape. This is the first report to reveal the morphogenesis of iSSLs from the shape of the crypt.
Keywords: depressed surface; endophytic growth; frustoconical crypt; inverted sessile serrated lesions; serrated polyposis syndrome.
© 2021 The Authors. DEN Open published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Dekker E, Bleijenberg A, Balaguer F. Update on the world Health organization criteria for diagnosis of serrated polyposis syndrome. Gastroenterology 2020; 158: 1520–3. - PubMed
-
- Uraoka T, Saito Y, Ikematsu H, Yamamoto K, Sano Y. Sano's capillary pattern classification for narrow‐band imaging of early colorectal lesions. Dig Endosc 2011; 23 (Suppl 1): 112–5. - PubMed
-
- Kimura T, Yamamoto E, Yamano HO, et al. A novel pit pattern identifies the precursor of colorectal cancer derived from sessile serrated adenoma. Am J Gastroenterol 2012; 107: 460–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources