

Efficacy of endoscopic retrograde cholangiopancreatography in familial adenomatous polyposis patients after duodenectomy
- PMID: 35310730
- PMCID: PMC8828246
- DOI: 10.1002/deo2.85
Efficacy of endoscopic retrograde cholangiopancreatography in familial adenomatous polyposis patients after duodenectomy
Abstract
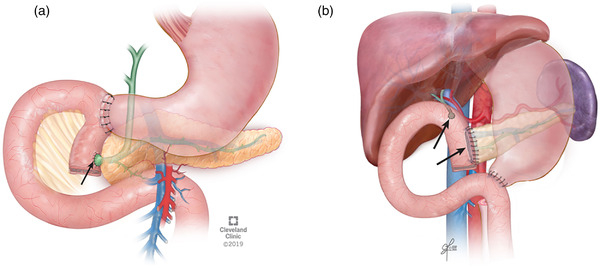
Objectives: Familial adenomatous polyposis (FAP) patients with Spigelman stage IV polyposis should be considered for prophylactic duodenectomy. Post-surgical pancreaticobiliary complications occur and may require management via endoscopic retrograde cholangiopancreatography (ERCP). We aimed to assess the success and adverse events of ERCP in FAP patients after pancreas-sparing duodenectomy (PSD) and pancreaticoduodenectomy (PD).
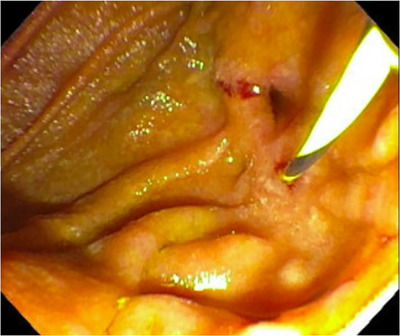
Methods: A retrospective review of FAP patients who underwent ERCP after PSD or PD from 1992 to 2020 at a quaternary referral center was completed. The technical success of ERCP was defined as the ability to identify the anastomosis and cannulate the duct. Post-procedural adverse events were defined by bleeding, perforation, pancreatitis, or cholangitis. Clinical outcomes included the need for surgical intervention and recurrent pancreatitis after ERCP were assessed.
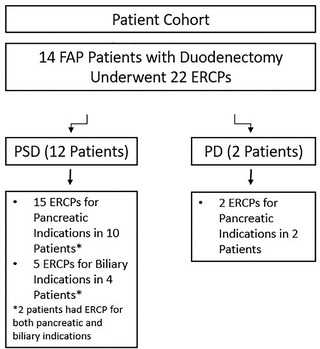
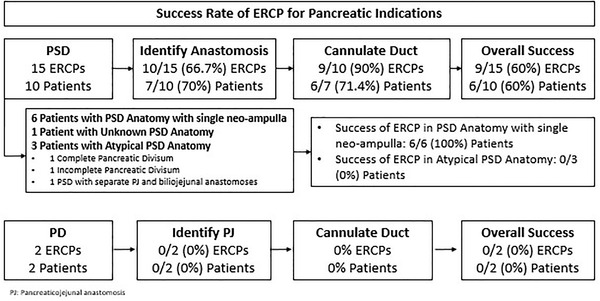
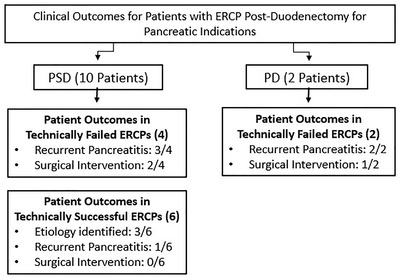
Results: Of 84 FAP patients with duodenectomy, 12 patients with PSD and two patients with PD underwent 17 ERCPs for pancreatic indications and five for biliary indications. The technical success of ERCP in patients with PSD and a single neoampullary complex for pancreatic (n = 6) and biliary (n = 5) indications was 100% but for those with PD (n = 2) or PSD reconstruction with pancreatic divisum or separate anastomoses (n = 3), it was 0%. Surgical intervention was required in 50% of patients with technically failed ERCP after PSD (2/4) and PD (1/2). There were no adverse events.
Conclusions: ERCP is expected to be therapeutically successful for biliary complications following PSD. Assessment and potential therapy for pancreatitis post-PSD are best in the setting of a single neo-ampullary complex rather than in PD or PSD with pancreatic divisum.
Keywords: adenomatous polyposis coli; cholangiopancreatography; endoscopic retrograde; endoscopy; gastrointestinal; pancreaticoduodenectomy; pancreatitis.
© 2022 The Authors. DEN Open published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
Carol A. Burke has no relevant disclosures but has research support from Janssen Pharmaceuticals, Ferring Pharmaceuticals, and Cancer Prevention Pharmaceuticals and consulting fees from Freenome, Ferring Pharmaceuticals, and SLA Pharma. Amit Bhatt has no relevant disclosures but has royalties from Medtronics and consulting fees from Boston Scientific, Lumendi, Steris, Intuitive. All other authors do not have any conflict of interest.
Figures

Similar articles
-
Laparoscopic Pancreas-Sparing Duodenectomy with Roux en Y Reconstruction for Duodenal Polyposis.Chirurgia (Bucur). 2019 Jul-Aug;114(4):494-505. doi: 10.21614/chirurgia.114.4.502. Chirurgia (Bucur). 2019. PMID: 31511136
-
The Prevalence and Significance of Jejunal and Duodenal Bulb Polyposis After Duodenectomy in Familial Adenomatous Polyposis: Retrospective Cohort Study.Ann Surg. 2021 Dec 1;274(6):e1071-e1077. doi: 10.1097/SLA.0000000000003740. Ann Surg. 2021. PMID: 31850977
-
Long-Term Outcomes of Pancreas-Sparing Duodenectomy for Duodenal Polyposis in Familial Adenomatous Polyposis Syndrome.J Gastrointest Surg. 2021 May;25(5):1233-1240. doi: 10.1007/s11605-020-04621-7. Epub 2020 May 14. J Gastrointest Surg. 2021. PMID: 32410179
-
The role of endoscopic retrograde cholangiopancreatography and endoscopic ultrasound in diagnosis and treatment of acute pancreatitis.Minerva Gastroenterol Dietol. 2005 Dec;51(4):265-88. Minerva Gastroenterol Dietol. 2005. PMID: 16282957 Review.
-
Selective biliary cannulation techniques for endoscopic retrograde cholangiopancreatography procedures and prevention of post- endoscopic retrograde cholangiopancreatography pancreatitis.Expert Rev Gastroenterol Hepatol. 2016 Jun;10(6):709-22. doi: 10.1586/17474124.2016.1143774. Epub 2016 Feb 6. Expert Rev Gastroenterol Hepatol. 2016. PMID: 26782710 Review.
References
-
- Yang J, Gurudu SR, Koptiuch C et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in familial adenomatous polyposis syndromes. Gastrointest endosc 2020; 91: 963–82.e2. - PubMed
-
- van Leerdam ME, Roos VH, van Hooft JE et al. Endoscopic management of polyposis syndromes: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2019; 51: 877–95. - PubMed
-
- Johnson MD, Mackey R, Brown N, Church J, Burke C, Walsh RM. Outcome based on management for duodenal adenomas: Sporadic versus familial disease. J Gastrointest Surg 2010; 14: 229–35. - PubMed
-
- Thiruvengadam SS, Lopez R, O'Malley M et al. Spigelman stage IV duodenal polyposis does not precede most duodenal cancer cases in patients with familial adenomatous polyposis. Gastrointest Endosc 2019; 89: 345–54.e2. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous