

Endoscopic ultrasonography-guided tissue acquisition for small solid pancreatic lesions: Does the size matter?
- PMID: 35310760
- PMCID: PMC8828213
- DOI: 10.1002/deo2.52
Endoscopic ultrasonography-guided tissue acquisition for small solid pancreatic lesions: Does the size matter?
Abstract
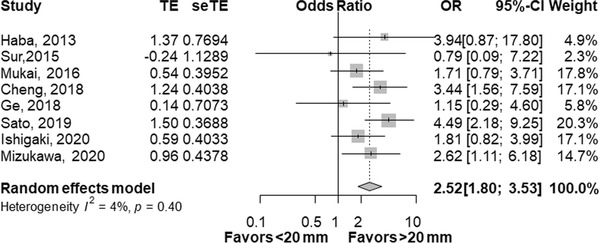
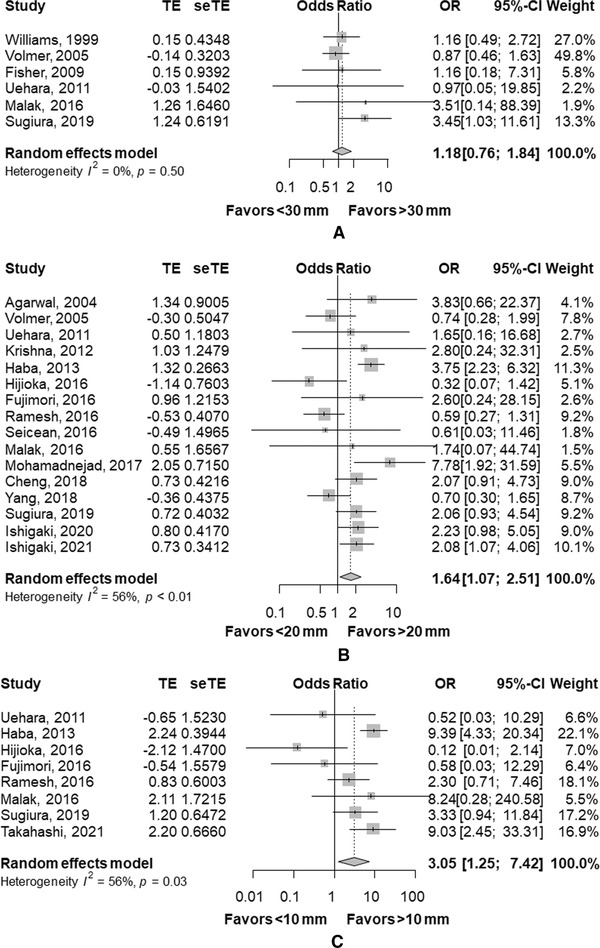
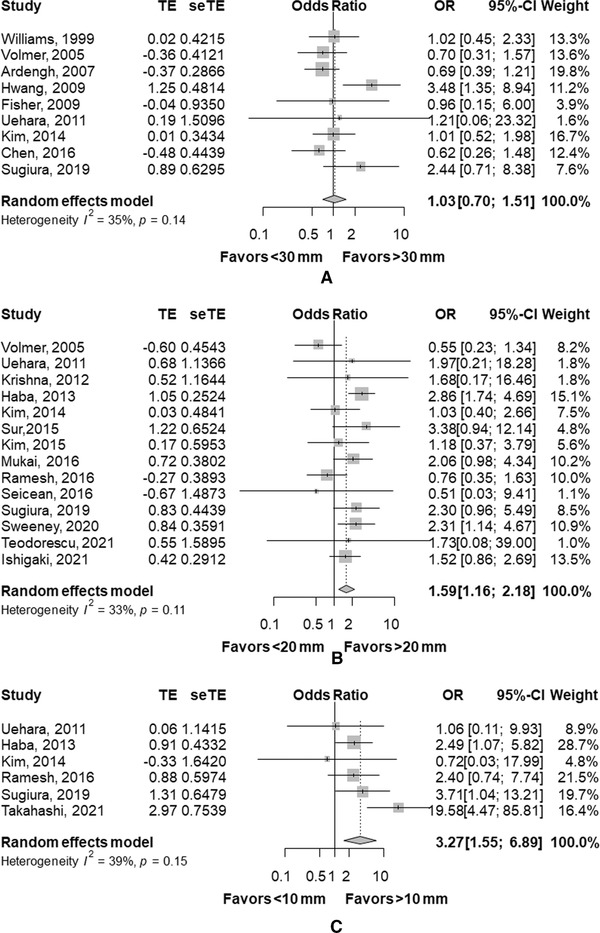
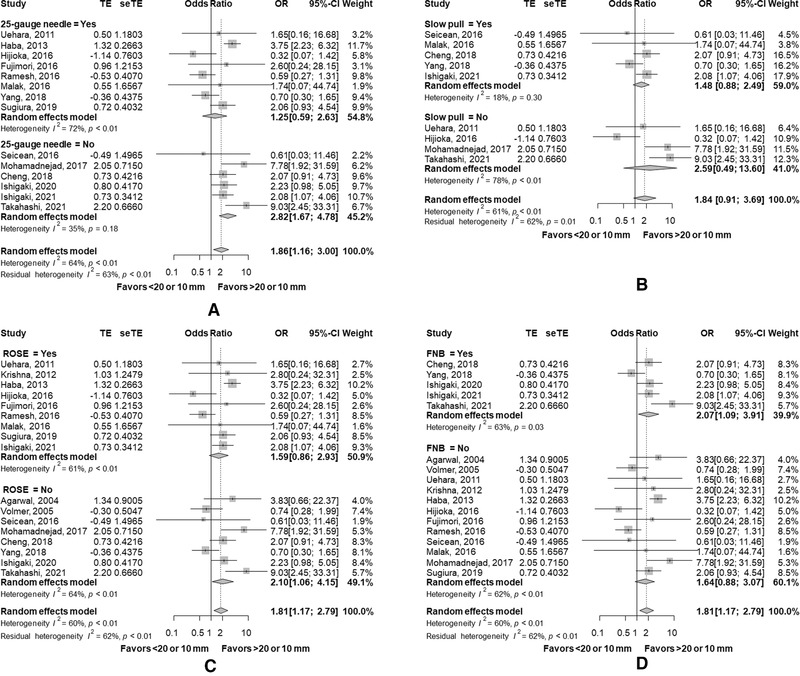
Endoscopic ultrasonography-guided tissue acquisition (EUS-TA) is now an established technique to obtain the pathological diagnosis of solid pancreatic lesions (SPLs), but the diagnosis of small SPLS by EUS-TA can still be difficult. We conducted a literature review and a meta-analysis on the diagnostic yield of EUS-TA according to the tumor size. In a meta-analysis of 33 studies with 6883 cases, a pooled odds ratio (OR) of sensitivity was significantly higher in SPLs of >20 mm (OR 1.64, p = 0.02) and in SPLs of >10 mm (OR 3.05, p = 0.01), but not in SPLs of >30 mm (OR 1.18, p = 0.46). The meta-analysis of accuracy also showed a similar trend: OR of 1.59 in SPLs of >20 mm (p < 0.01) and OR of 3.27 in SPLs of >10 mm (p < 0.01) and OR of 1.03 in SPLs of >30 mm (p = 0.87). The use of a 25-gauge needle tended to improve sensitivity in small SPLs, though not statistically significant: OR of 1.25 and 2.82 in studies with and without a 25-gauge needle (p = 0.08). The use of fine needle biopsy needles, slow pull method, and rapid on-site evaluation did not significantly improve sensitivity in small SPLs. EUS-TA for small SPLs, especially neuroendocrine neoplasms, is reported to have a high risk of adverse events. In summary, the diagnostic yield and safety of EUS-TA for small (<20 mm) SPLs still needs improvement, and the best needle and technique for small SPLs should be further investigated.
Keywords: endoscopic ultrasound; fine needle aspiration; fine needle biopsy; pancreatic lesions.
© 2021 The Authors. DEN Open published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
Yousuke Nakai receivedresearch grant from Boston Scientific Japan, Fujifilm Corporation, HOYA Corporation, Medico's Hirata and honoraria from Boston Scientific Japan, Fujifilm Corporation, Medico's Hirata, Medtronic, Olympus Corporation. Hirofumi Kogure received honoraria from Boston Scientific Japan, Fujifilm Corporation, Medico's Hirata, and Olympus Corporation. Mitsuhiro Fujishir received research grant from Fujifilm Corporation, HOYA Corporation, Olympus Corporation and honoraria from Fujifilm Corporation and Olympus Corporation. Yousuke Nakai is an associate editor of digestive endoscopy.
Figures
Similar articles
-
EUS-guided reverse bevel fine-needle biopsy sampling and open tip fine-needle aspiration in solid pancreatic lesions - a prospective, comparative study.Scand J Gastroenterol. 2018 Feb;53(2):231-237. doi: 10.1080/00365521.2017.1421704. Epub 2018 Jan 4. Scand J Gastroenterol. 2018. PMID: 29301477 Clinical Trial.
-
Diagnostic performance of EUS-guided tissue acquisition for solid pancreatic lesions ≤10 mm.Endosc Ultrasound. 2024 Mar-Apr;13(2):115-122. doi: 10.1097/eus.0000000000000052. Epub 2024 Apr 5. Endosc Ultrasound. 2024. PMID: 38947747 Free PMC article.
-
Touch imprint cytology on endoscopic ultrasound fine-needle biopsy provides comparable sample quality and diagnostic yield to standard endoscopic ultrasound fine-needle aspiration specimens in the evaluation of solid pancreatic lesions.Cytopathology. 2019 Mar;30(2):179-186. doi: 10.1111/cyt.12662. Epub 2018 Dec 21. Cytopathology. 2019. PMID: 30484917
-
The Utility of Endoscopic-Ultrasonography-Guided Tissue Acquisition for Solid Pancreatic Lesions.Diagnostics (Basel). 2022 Mar 19;12(3):753. doi: 10.3390/diagnostics12030753. Diagnostics (Basel). 2022. PMID: 35328306 Free PMC article. Review.
-
Endoscopic ultrasound fine needle aspiration vs fine needle biopsy for pancreatic masses, subepithelial lesions, and lymph nodes.World J Gastroenterol. 2021 Jul 14;27(26):4194-4207. doi: 10.3748/wjg.v27.i26.4194. World J Gastroenterol. 2021. PMID: 34326619 Free PMC article. Review.
Cited by
-
EUS-FNA versus EUS-FNB in Pancreatic Solid Lesions ≤ 15 mm.Diagnostics (Basel). 2024 Feb 15;14(4):427. doi: 10.3390/diagnostics14040427. Diagnostics (Basel). 2024. PMID: 38396466 Free PMC article.
-
Comparison of Diagnostic Yield and Safety of Serial Pancreatic Juice Aspiration Cytologic Examination (SPACE) with Different Indications.Diagnostics (Basel). 2023 Apr 21;13(8):1498. doi: 10.3390/diagnostics13081498. Diagnostics (Basel). 2023. PMID: 37189599 Free PMC article.
-
The outcomes of endoscopic ultrasound-guided tissue acquisition for small focal liver lesions measuring ≤2 cm.DEN Open. 2024 Oct 21;5(1):e70031. doi: 10.1002/deo2.70031. eCollection 2025 Apr. DEN Open. 2024. PMID: 39439546 Free PMC article.
-
Effectiveness of endoscopic ultrasound-guided tissue acquisition with stereomicroscopic on-site evaluation for preoperative diagnosis of resectable or borderline resectable pancreatic cancer: a prospective study.Clin Endosc. 2024 Nov;57(6):807-813. doi: 10.5946/ce.2023.277. Epub 2024 May 24. Clin Endosc. 2024. PMID: 38919058 Free PMC article.
-
The impact of biliary stents on the diagnostic yield of endoscopic ultrasound-guided fine needle aspiration for solid pancreatic lesions: A single-center retrospective study and meta-analysis.DEN Open. 2023 Jul 10;4(1):e250. doi: 10.1002/deo2.250. eCollection 2024 Apr. DEN Open. 2023. PMID: 37441156 Free PMC article.
References
-
- Vilmann P, Jacobsen GK, Henriksen FW, Hancke S. Endoscopic ultrasonography with guided fine needle aspiration biopsy in pancreatic disease. Gastrointest Endosc 1992; 38: 172–3. - PubMed
-
- Chang KJ, Albers CG, Erickson RA, Butler JA, Wuerker RB, Lin F. Endoscopic ultrasound‐guided fine needle aspiration of pancreatic carcinoma. Am J Gastroenterol 1994; 89: 263–6. - PubMed
-
- Bang JY, Kirtane S, Krall K, et al. In memoriam: Fine‐needle aspiration, birth: Fine‐needle biopsy: The changing trend in endoscopic ultrasound‐guided tissue acquisition. Dig Endosc 2019; 31: 197–202. - PubMed
Publication types
LinkOut - more resources
Full Text Sources