

Efficacy and Safety of Veno-Arterial Extracorporeal Membrane Oxygenation in the Treatment of High-Risk Pulmonary Embolism: A Retrospective Cohort Study
- PMID: 35310966
- PMCID: PMC8924067
- DOI: 10.3389/fcvm.2022.799488
Efficacy and Safety of Veno-Arterial Extracorporeal Membrane Oxygenation in the Treatment of High-Risk Pulmonary Embolism: A Retrospective Cohort Study
Abstract
Objectives: Veno-arterial extracorporeal membrane oxygenation (ECMO) is increasingly used to treat high-risk pulmonary embolism (PE). However, its efficacy and safety remain uncertain. This retrospective cohort study aimed to determine whether ECMO could improve the clinical outcomes of patients with high-risk PE.
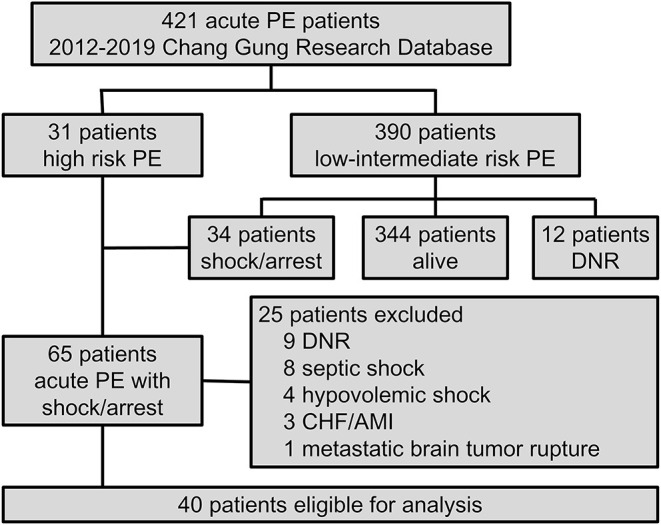
Methods: Forty patients with high-risk PE, who were admitted to Kaohsiung Chang Gung Memorial Hospital between January 2012 and December 2019, were included in this study. Demographic data and clinical outcomes were compared between patients treated without ECMO (non-ECMO group) and those treated with ECMO (ECMO group). Appropriate statistical tools were used to compare variables between groups and the survival was analyzed using the Kaplan-Meier method.
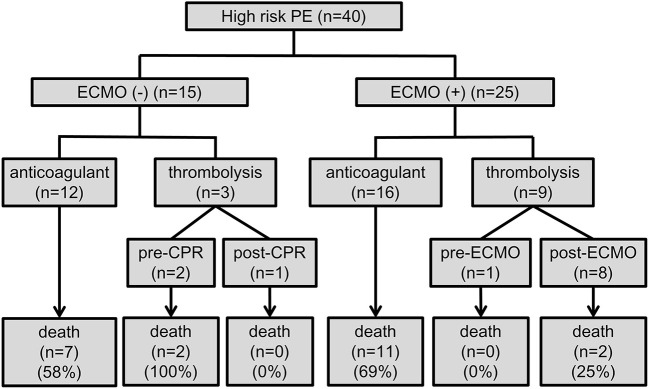
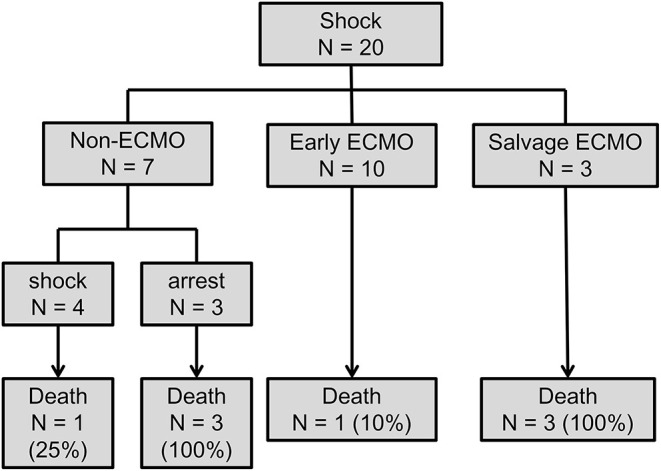
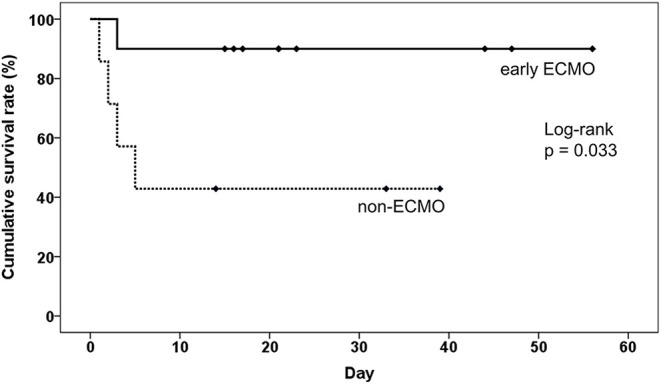
Results: The overall in-hospital mortality rate was 55%, in which 65% (26/40) of patients presented with cardiac arrest with a mortality rate of 77%, which was higher than that of patients without cardiac arrest (14%). There was no significant difference in major complications and in-hospital mortality between the non-ECMO and ECMO groups. However, in subgroup analysis, compared with patients treated without ECMO, earlier ECMO treatment was associated with a reduced risk of cardiac arrest (P = 0.023) and lower in-hospital mortality (P = 0.036). A log-rank test showed a significantly higher cumulative overall survival in the earlier ECMO treatment group (P = 0.033).
Conclusions: In this retrospective cohort study, earlier ECMO treatment was associated with lower in-hospital mortality among unstable patients without cardiac arrest. Our findings suggest that ECMO can be considered as an initial treatment option for patients with high-risk PE in higher-volume hospitals.
Keywords: ECMO; cardiac arrest; pulmonary embolism; shock; sudden death.
Copyright © 2022 Tsai, Wang, Lee, Yen, Lo, Wu, Huang, Chen, Sheu and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical course and outcome of patients with acute pulmonary embolism rescued by veno-arterial extracorporeal membrane oxygenation: a retrospective review of 21 cases.J Cardiothorac Surg. 2020 Oct 2;15(1):295. doi: 10.1186/s13019-020-01347-0. J Cardiothorac Surg. 2020. PMID: 33008478 Free PMC article.
-
Mid-term outcomes with the use of extracorporeal membrane oxygenation for cardiopulmonary failure secondary to massive pulmonary embolism.Eur J Cardiothorac Surg. 2020 Nov 1;58(5):923-931. doi: 10.1093/ejcts/ezaa189. Eur J Cardiothorac Surg. 2020. PMID: 32725134
-
A retrospective comparison of survivors and non-survivors of massive pulmonary embolism receiving veno-arterial extracorporeal membrane oxygenation support.Resuscitation. 2018 Jan;122:1-5. doi: 10.1016/j.resuscitation.2017.11.034. Epub 2017 Nov 8. Resuscitation. 2018. PMID: 29128608
-
Survival of patients with acute pulmonary embolism treated with venoarterial extracorporeal membrane oxygenation: A systematic review and meta-analysis.J Crit Care. 2021 Aug;64:245-254. doi: 10.1016/j.jcrc.2021.03.006. Epub 2021 Mar 24. J Crit Care. 2021. PMID: 34049258
-
Use of extracorporeal membrane oxygenation in high-risk acute pulmonary embolism: A systematic review and meta-analysis.Artif Organs. 2021 Jun;45(6):569-576. doi: 10.1111/aor.13876. Epub 2021 Jan 10. Artif Organs. 2021. PMID: 33277695
Cited by
-
Extracorporeal membrane oxygenation for large pulmonary emboli.Proc (Bayl Univ Med Cent). 2023 Feb 9;36(3):314-317. doi: 10.1080/08998280.2023.2171699. eCollection 2023. Proc (Bayl Univ Med Cent). 2023. PMID: 37091759 Free PMC article.
-
Extracorporeal Membrane Oxygenation (ECMO): A Lifeline for Pregnant and Postpartum Women.Cureus. 2023 Aug 16;15(8):e43586. doi: 10.7759/cureus.43586. eCollection 2023 Aug. Cureus. 2023. PMID: 37719551 Free PMC article. Review.
-
Survival after venoarterial extracorporeal membrane oxygenation for acute high-risk Pulmonary Embolism: A meta-analysis of comparative studies.Pak J Med Sci. 2025 Jan;41(1):312-317. doi: 10.12669/pjms.41.1.10568. Pak J Med Sci. 2025. PMID: 39867790 Free PMC article. Review.
-
The use of Veno-arterial Extracorporeal Membrane Oxygenation (VA-ECMO) for Acute High Risk Pulmonary Embolism: A Systematic Review.Curr Cardiol Rev. 2025;21(4):e1573403X339627. doi: 10.2174/011573403X339627241224085451. Curr Cardiol Rev. 2025. PMID: 40525417
-
Extracorporeal Membrane Oxygenation for Pulmonary Embolism: A Systematic Review and Meta-Analysis.J Clin Med. 2023 Dec 22;13(1):64. doi: 10.3390/jcm13010064. J Clin Med. 2023. PMID: 38202071 Free PMC article. Review.
References
-
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. . 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. (2020) 41:543–603. 10.1093/eurheartj/ehz405 - DOI - PubMed
LinkOut - more resources
Full Text Sources