

Surgical Treatment for Colorectal Cancer Partially Restores Gut Microbiome and Metabolome Traits
- PMID: 35311577
- PMCID: PMC9040882
- DOI: 10.1128/msystems.00018-22
Surgical Treatment for Colorectal Cancer Partially Restores Gut Microbiome and Metabolome Traits
Abstract
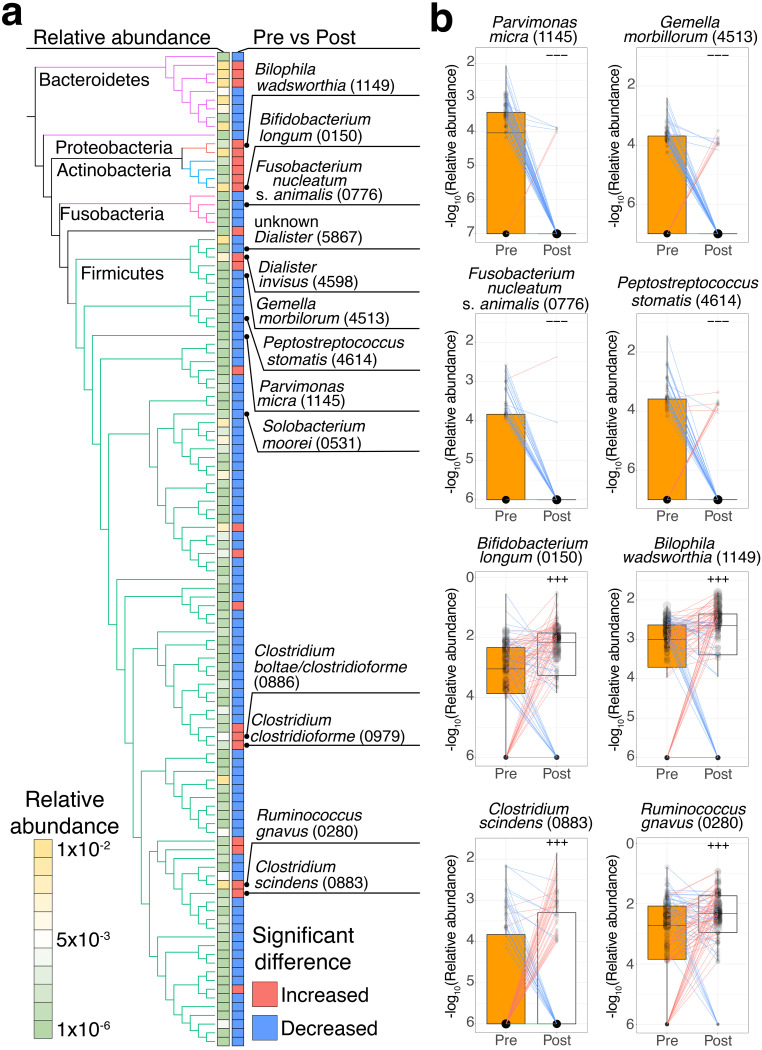
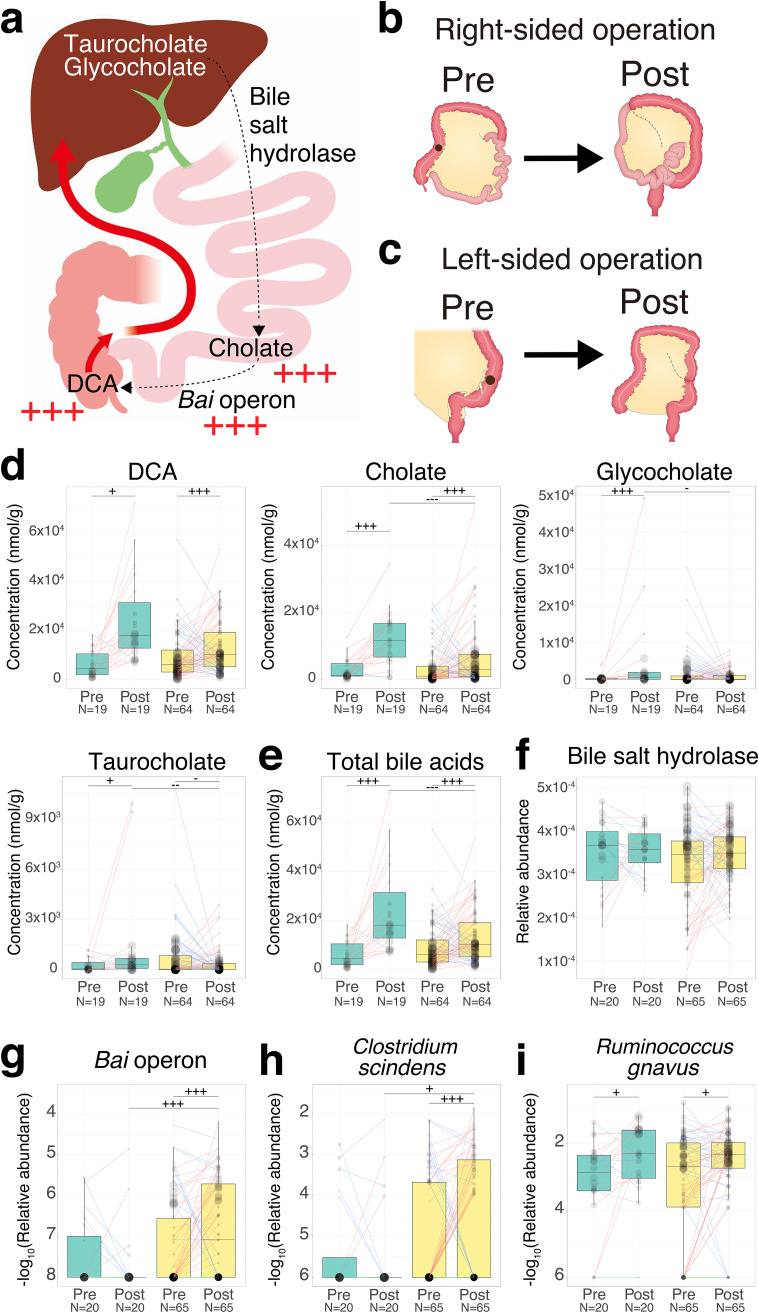
Accumulating evidence indicates that the gut microbiome and metabolites are associated with colorectal cancer (CRC). However, the influence of surgery for CRC treatment on the gut microbiome and metabolites and how it relates to CRC risk in postoperative CRC patients remain partially understood. Here, we collected 170 fecal samples from 85 CRC patients pre- and approximately 1 year postsurgery and performed shotgun metagenomic sequencing and capillary electrophoresis-time of flight mass spectrometry-based metabolomics analyses to characterize alterations between pre- and postsurgery. We determined that the relative abundance of 114 species was altered postsurgery (P < 0.005). CRC-associated species, such as Fusobacterium nucleatum, were decreased postsurgery. On the other hand, Clostridium scindens, carcinogenesis-associated deoxycholate (DCA)-producing species, and its biotransformed genes (bai operon) were increased postsurgery. The concentration of 60 fecal metabolites was also altered postsurgery (P < 0.005). Two bile acids, cholate and DCA, were increased postsurgery. We developed methods to estimate postoperative CRC risk based on the gut microbiome and metabolomic compositions using a random forest machine-learning algorithm that classifies large adenoma or early-stage CRC and healthy controls from publicly available data sets. We applied methods to preoperative samples and then compared the estimated CRC risk between the two groups according to the presence of large adenoma or tumors 5 years postsurgery (P < 0.05). Overall, our results show that the gut microbiome and metabolites dynamically change from pre- to postsurgery. In postoperative CRC patients, potential CRC risk derived from gut microbiome and metabolites still remains, which indicates the importance of follow-up assessments. IMPORTANCE The gut microbiome and metabolites are associated with CRC progression and carcinogenesis. Postoperative CRC patients are reported to be at an increased CRC risk; however, how gut microbiome and metabolites are related to CRC risk in postoperative patients remains only partially understood. In this study, we investigated the influence of surgical CRC treatment on the gut microbiome and metabolites. We found that the CRC-associated species Fusobacterium nucleatum was decreased postsurgery, whereas carcinogenesis-associated DCA and its producing species and genes were increased postsurgery. We developed methods to estimate postoperative CRC risk based on the gut microbiome and metabolomic compositions. We applied methods to compare the estimated CRC risk between two groups according to the presence of large adenoma or tumors after 5 years postsurgery. To our knowledge, this study is the first report on differences between pre- and postsurgery using metagenomics and metabolomics data analysis. Our methods might be used for CRC risk assessment in postoperative patients.
Keywords: colorectal cancer; human gut microbiome; metabolomics; metagenomics; surgery.
Conflict of interest statement
The authors declare a conflict of interest. Dr. Shinji Fukuda and Dr. Takuji Yamada are founders of Metabologenomics. The company is focused on the design and control of the gut environment for human health. The company had no control over the interpretation, writing or publication of this work. The terms of these arrangements are being managed by Keio University and Tokyo Institute of Technology according to their conflict of interest policies.
Figures




Similar articles
-
Fecal Metabolomic Signatures in Colorectal Adenoma Patients Are Associated with Gut Microbiota and Early Events of Colorectal Cancer Pathogenesis.mBio. 2020 Feb 18;11(1):e03186-19. doi: 10.1128/mBio.03186-19. mBio. 2020. PMID: 32071266 Free PMC article.
-
Integrated analysis of the faecal metagenome and serum metabolome reveals the role of gut microbiome-associated metabolites in the detection of colorectal cancer and adenoma.Gut. 2022 Jul;71(7):1315-1325. doi: 10.1136/gutjnl-2020-323476. Epub 2021 Aug 30. Gut. 2022. PMID: 34462336 Free PMC article.
-
Altered gut metabolites and microbiota interactions are implicated in colorectal carcinogenesis and can be non-invasive diagnostic biomarkers.Microbiome. 2022 Feb 21;10(1):35. doi: 10.1186/s40168-021-01208-5. Microbiome. 2022. PMID: 35189961 Free PMC article.
-
Significance of the gut microbiome in multistep colorectal carcinogenesis.Cancer Sci. 2020 Mar;111(3):766-773. doi: 10.1111/cas.14298. Epub 2020 Feb 3. Cancer Sci. 2020. PMID: 31910311 Free PMC article. Review.
-
Progress of gut microbiome and its metabolomics in early screening of colorectal cancer.Clin Transl Oncol. 2023 Jul;25(7):1949-1962. doi: 10.1007/s12094-023-03097-6. Epub 2023 Feb 15. Clin Transl Oncol. 2023. PMID: 36790675 Review.
Cited by
-
Colorectal microbiota after removal of colorectal cancer.NAR Cancer. 2022 Apr 8;4(2):zcac011. doi: 10.1093/narcan/zcac011. eCollection 2022 Jun. NAR Cancer. 2022. PMID: 35399186 Free PMC article.
-
Baseline gut microbiome alpha diversity predicts chemotherapy-induced gastrointestinal symptoms in patients with breast cancer.NPJ Breast Cancer. 2024 Nov 15;10(1):99. doi: 10.1038/s41523-024-00707-6. NPJ Breast Cancer. 2024. PMID: 39548124 Free PMC article.
-
Microbiome and Colorectal Cancer in Humans: A Review of Recent Studies.J Anus Rectum Colon. 2025 Jan 25;9(1):20-24. doi: 10.23922/jarc.2024-080. eCollection 2025. J Anus Rectum Colon. 2025. PMID: 39882224 Free PMC article. Review.
References
-
- Kakeji Y, Takahashi A, Udagawa H, Unno M, Endo I, Kunisaki C, Taketomi A, Tangoku A, Masaki T, Marubashi S, Yoshida K, Gotoh M, Konno H, Miyata H, Seto Y, National Clinical Database. 2018. Surgical outcomes in gastroenterological surgery in Japan: report of National Clinical database 2011–2016. Ann Gastroenterol Surg 2:37–54. doi:10.1002/ags3.12052. - DOI - PMC - PubMed
-
- Yabuuchi Y, Imai K, Hotta K, Ito S, Kishida Y, Yamaguchi T, Shiomi A, Kinugasa Y, Yoshida M, Tanaka M, Kawata N, Kakushima N, Takizawa K, Ishiwatari H, Matsubayashi H, Ono H. 2018. Higher incidence of metachronous advanced neoplasia in patients with synchronous advanced neoplasia and left-sided colorectal resection for colorectal cancer. Gastrointest Endosc 88:348–359.e1. doi:10.1016/j.gie.2018.03.011. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
