

A multi-modal exploration of heterogeneous physico-chemical properties of DCIS breast microcalcifications
- PMID: 35311860
- PMCID: PMC8997374
- DOI: 10.1039/d1an01548f
A multi-modal exploration of heterogeneous physico-chemical properties of DCIS breast microcalcifications
Abstract
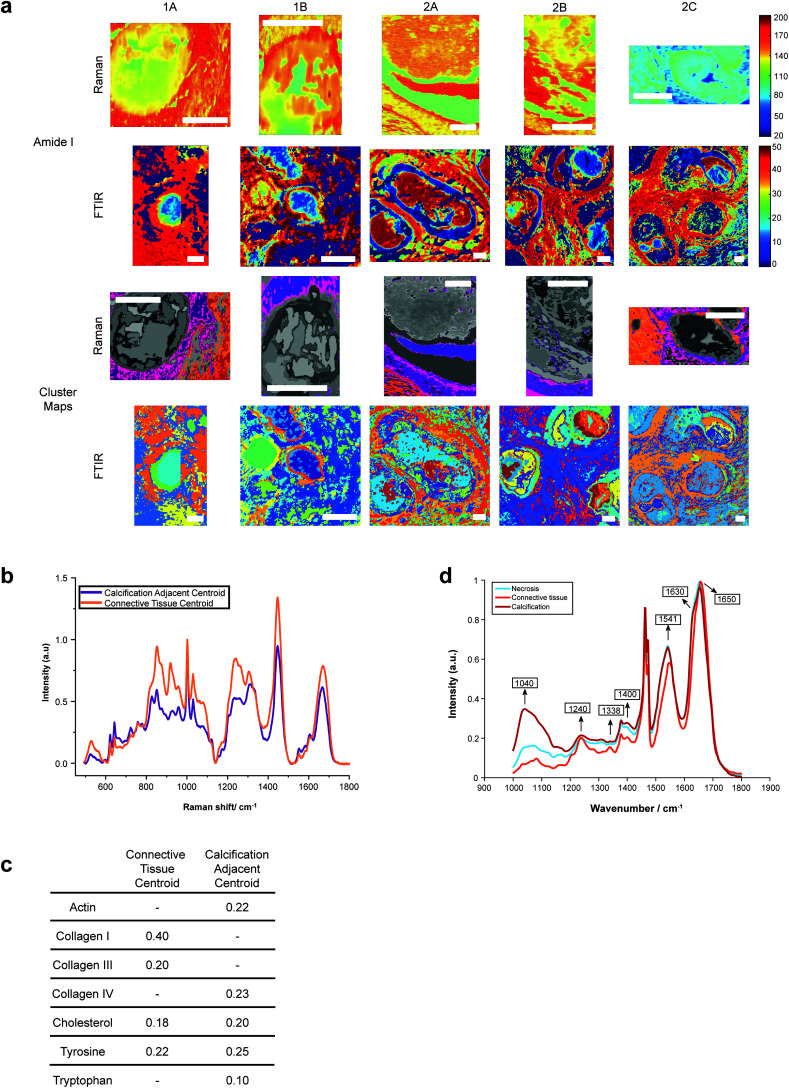
Ductal carcinoma in situ (DCIS) is frequently associated with breast calcification. This study combines multiple analytical techniques to investigate the heterogeneity of these calcifications at the micrometre scale. X-ray diffraction, scanning electron microscopy and Raman and Fourier-transform infrared spectroscopy were used to determine the physicochemical and crystallographic properties of type II breast calcifications located in formalin fixed paraffin embedded DCIS breast tissue samples. Multiple calcium phosphate phases were identified across the calcifications, distributed in different patterns. Hydroxyapatite was the dominant mineral, with magnesium whitlockite found at the calcification edge. Amorphous calcium phosphate and octacalcium phosphate were also identified close to the calcification edge at the apparent mineral/matrix barrier. Crystallographic features of hydroxyapatite also varied across the calcifications, with higher crystallinity centrally, and highest carbonate substitution at the calcification edge. Protein was also differentially distributed across the calcification and the surrounding soft tissue, with collagen and β-pleated protein features present to differing extents. Combination of analytical techniques in this study was essential to understand the heterogeneity of breast calcifications and how this may link crystallographic and physicochemical properties of calcifications to the surrounding tissue microenvironment.
Conflict of interest statement
There are no conflicts to declare.
Figures





Similar articles
-
Microcalcification crystallography as a potential marker of DCIS recurrence.Sci Rep. 2023 Jun 8;13(1):9331. doi: 10.1038/s41598-023-33547-8. Sci Rep. 2023. PMID: 37291276 Free PMC article.
-
Calcification Microstructure Reflects Breast Tissue Microenvironment.J Mammary Gland Biol Neoplasia. 2019 Dec;24(4):333-342. doi: 10.1007/s10911-019-09441-3. Epub 2019 Dec 5. J Mammary Gland Biol Neoplasia. 2019. PMID: 31807966 Free PMC article.
-
Qualitative Radiogenomics: Association Between BI-RADS Calcification Descriptors and Recurrence Risk as Assessed by the Oncotype DX Ductal Carcinoma In Situ Score.AJR Am J Roentgenol. 2019 Apr;212(4):919-924. doi: 10.2214/AJR.18.20306. Epub 2019 Feb 4. AJR Am J Roentgenol. 2019. PMID: 30714832
-
[The role of breast magnetic resonance imaging in the diagnosis of ductal carcinoma in situ].Srp Arh Celok Lek. 2013 May-Jun;141(5-6):402-8. doi: 10.2298/sarh1306402n. Srp Arh Celok Lek. 2013. PMID: 23858817 Review. Serbian.
-
Intratumoral Heterogeneity in Ductal Carcinoma In Situ: Chaos and Consequence.J Mammary Gland Biol Neoplasia. 2018 Dec;23(4):191-205. doi: 10.1007/s10911-018-9410-6. Epub 2018 Sep 7. J Mammary Gland Biol Neoplasia. 2018. PMID: 30194658 Free PMC article. Review.
Cited by
-
Mechanisms of osteopontin-stabilized amorphous calcium phosphate calcification in benign and pre-malignant breast disease.Sci Rep. 2025 Jul 4;15(1):23849. doi: 10.1038/s41598-025-08903-5. Sci Rep. 2025. PMID: 40615470 Free PMC article.
-
Characterization of dolomite and calcite microcalcifications in human breast tissue.RSC Adv. 2024 Sep 10;14(39):28741-28752. doi: 10.1039/d4ra04137b. eCollection 2024 Sep 4. RSC Adv. 2024. PMID: 39257663 Free PMC article.
-
Microcalcification crystallography as a potential marker of DCIS recurrence.Sci Rep. 2023 Jun 8;13(1):9331. doi: 10.1038/s41598-023-33547-8. Sci Rep. 2023. PMID: 37291276 Free PMC article.
-
Prostate microcalcification crystallography as a marker of pathology.Sci Rep. 2025 Apr 29;15(1):14979. doi: 10.1038/s41598-025-98692-8. Sci Rep. 2025. PMID: 40301587 Free PMC article.
-
Exploration of utility of combined optical photothermal infrared and Raman imaging for investigating the chemical composition of microcalcifications in breast cancer.Anal Methods. 2023 Mar 30;15(13):1620-1630. doi: 10.1039/d2ay01197b. Anal Methods. 2023. PMID: 36880909 Free PMC article.
References
-
- Frappart L. Boudeulle M. Boumendil J. Lin H. C. Martinon I. Palayer C. et al., Structure and composition of microcalcifications in benign and malignant lesions of the breast: Study by light microscopy, transmission and scanning electron microscopy, microprobe analysis, and X-ray diffraction. Hum. Pathol. 1984;15:880–889. doi: 10.1016/S0046-8177(84)80150-1. - DOI - PubMed
-
- van Seijen M. Lips E. H. Fu L. Giardiello D. van Duijnhoven F. de Munck L. et al., Long-term risk of subsequent ipsilateral lesions after surgery with or without radiotherapy for ductal carcinoma in situ of the breast. Br. J. Cancer. 2021;125:1443–1449. doi: 10.1038/s41416-021-01496-6. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical