

Outcomes and Safety of History-Based Screening for Medication Abortion: A Retrospective Multicenter Cohort Study
- PMID: 35311911
- PMCID: PMC8938895
- DOI: 10.1001/jamainternmed.2022.0217
Outcomes and Safety of History-Based Screening for Medication Abortion: A Retrospective Multicenter Cohort Study
Abstract
Importance: Screening for medication abortion eligibility typically includes ultrasonography or pelvic examination. To reduce physical contact during the COVID-19 pandemic, many clinicians stopped requiring tests before medication abortion and instead screened patients for pregnancy duration and ectopic pregnancy risk by history alone. However, few US-based studies have been conducted on the outcomes and safety of this novel model of care.
Objective: To evaluate the outcomes and safety of a history-based screening, no-test approach to medication abortion care.
Design, setting, and participants: This retrospective cohort study included patients obtaining a medication abortion without preabortion ultrasonography or pelvic examination between February 1, 2020, and January 31, 2021, at 14 independent, Planned Parenthood, academic-affiliated, and online-only clinics throughout the US.
Exposures: Medications for abortion provided without preabortion ultrasonography or pelvic examination and dispensed to patients in person or by mail.
Main outcomes and measures: Effectiveness, defined as complete abortion after 200 μg of mifepristone and up to 1600 μg of misoprostol without additional intervention, and major abortion-related adverse events, defined as hospital admission, major surgery, or blood transfusion.
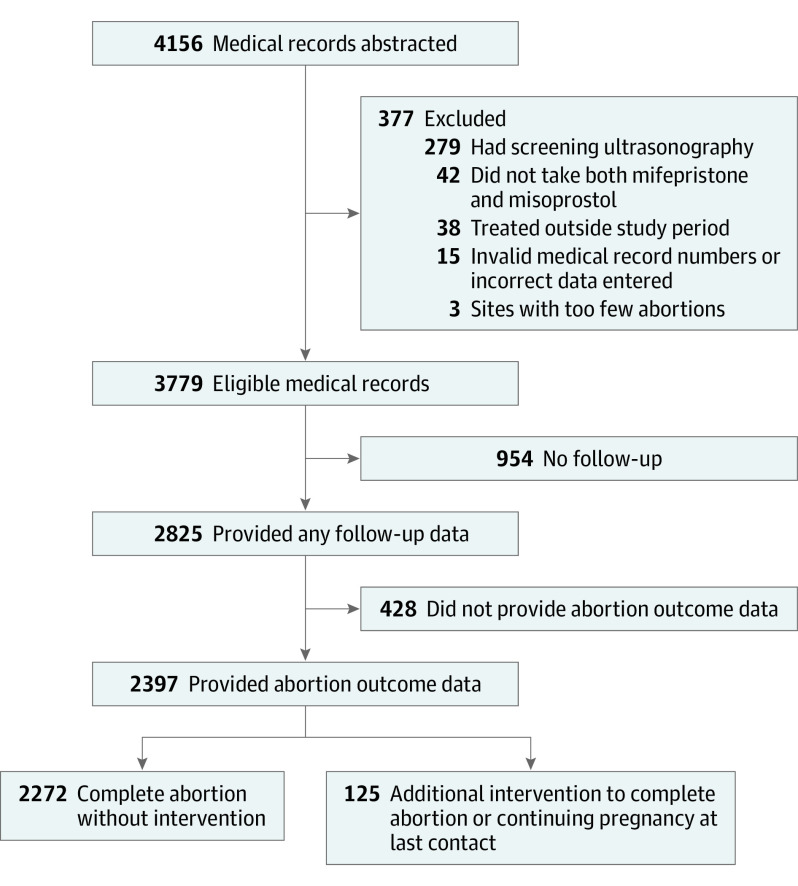
Results: The study included data on 3779 patients with eligible abortions. The study participants were racially and ethnically diverse and included 870 (23.0%) Black patients, 533 (14.1%) Latinx/Hispanic patients, 1623 (42.9%) White patients, and 327 (8.7%) who identified as multiracial or with other racial or ethnic groups. For most (2626 [69.5%]), it was their first medication abortion. Patients lived in 34 states, and 2785 (73.7%) lived in urban areas. In 2511 (66.4%) abortions, the medications were dispensed in person; in the other 1268 (33.6%), they were mailed to the patient. Follow-up data were obtained for 2825 abortions (74.8%), and multiple imputation was used to account for missing data. Across the sample, 12 abortions (0.54%; 95% CI, 0.18%-0.90%) were followed by major abortion-related adverse events, and 4 patients (0.22%; 95% CI, 0.00%-0.45%) were treated for ectopic pregnancies. Follow-up identified 9 (0.40%; 95% CI, 0.00%-0.84%) patients who had pregnancy durations of greater than 70 days on the date the mifepristone was dispensed that were not identified at screening. The adjusted effectiveness rate was 94.8% (95% CI, 93.6%-95.9%). Effectiveness was similar when medications were dispensed in person (95.4%; 95% CI, 94.1%-96.7%) or mailed (93.3%; 95% CI, 90.7%-95.9%).
Conclusions and relevance: In this cohort study, screening for medication abortion eligibility by history alone was effective and safe with either in-person dispensing or mailing of medications, resulting in outcomes similar to published rates of models involving ultrasonography or pelvic examination. This approach may facilitate more equitable access to this essential service by increasing the types of clinicians and locations offering abortion care.
Conflict of interest statement
Comment in
-
It Is Time to Change the Standard of Medication Abortion.JAMA Intern Med. 2022 May 1;182(5):491-493. doi: 10.1001/jamainternmed.2022.0216. JAMA Intern Med. 2022. PMID: 35311935 No abstract available.
Similar articles
-
Mail-Order Pharmacy Dispensing of Mifepristone for Medication Abortion After In-Person Screening.JAMA Intern Med. 2024 Aug 1;184(8):873-881. doi: 10.1001/jamainternmed.2024.1476. JAMA Intern Med. 2024. PMID: 38739404 Free PMC article.
-
Mailing abortion pills does not delay care: A cohort study comparing mailed to in-person dispensing of abortion medications in the United States.Contraception. 2023 May;121:109962. doi: 10.1016/j.contraception.2023.109962. Epub 2023 Feb 2. Contraception. 2023. PMID: 36736715 Free PMC article.
-
Comparison of No-Test Telehealth and In-Person Medication Abortion.JAMA. 2024 Sep 17;332(11):898-905. doi: 10.1001/jama.2024.10680. JAMA. 2024. PMID: 38913394 Free PMC article.
-
No-Test Medication Abortion: A Systematic Review.Obstet Gynecol. 2023 Jan 1;141(1):23-34. doi: 10.1097/AOG.0000000000005016. Epub 2022 Dec 5. Obstet Gynecol. 2023. PMID: 36701607
-
Medication abortion and uterine aspiration for undesired pregnancy of unknown location: A retrospective cohort study.Contraception. 2023 Jun;122:109980. doi: 10.1016/j.contraception.2023.109980. Epub 2023 Feb 16. Contraception. 2023. PMID: 36804050 Review.
Cited by
-
Abortion Training in Family Medicine Residency Programs: A National Survey of Program Directors 5 Months After the Dobbs Decision.Fam Med. 2024 Apr;56(4):242-249. doi: 10.22454/FamMed.2024.683874. Epub 2024 Jan 19. Fam Med. 2024. PMID: 38241748 Free PMC article.
-
Delays in Obtaining Abortion and Miscarriage Care Among Pregnant Persons in New York State During the COVID-19 Pandemic: The CAP Study.Womens Health Rep (New Rochelle). 2024 Jan 17;5(1):30-39. doi: 10.1089/whr.2023.0128. eCollection 2024. Womens Health Rep (New Rochelle). 2024. PMID: 38249936 Free PMC article.
-
Person-centered abortion care scale: Validation for medication abortion in the United States.Contraception. 2024 Sep;137:110485. doi: 10.1016/j.contraception.2024.110485. Epub 2024 May 15. Contraception. 2024. PMID: 38754758 Free PMC article.
-
Perceptions and experiences with two no-test direct-to-patient telehealth medication abortion regimens in the USA: an exploratory study with mifepristone and misoprostol and misoprostol-only regimens.BMJ Public Health. 2024 Oct 26;2(2):e000808. doi: 10.1136/bmjph-2023-000808. eCollection 2024 Dec. BMJ Public Health. 2024. PMID: 40018617 Free PMC article.
-
Nurse practitioners on 'the leading edge' of medication abortion care: A feminist qualitative approach.J Adv Nurs. 2023 Feb;79(2):686-697. doi: 10.1111/jan.15487. Epub 2022 Nov 11. J Adv Nurs. 2023. PMID: 36369652 Free PMC article.
References
-
- Jones RK, Witwer E, Jerman J, Jerman J. Abortion Incidence and Service Availability in the United States, 2017. Guttmacher Institute; 2019. doi:10.1363/2019.30760 - DOI
-
- Mifeprex (mifepristone) tablets, for oral use. Prescribing information. Danco Laboratories, LLC; 2016. Accessed November 6, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/020687s020lbl.pdf
-
- Planned Parenthood . The abortion pill. Accessed November 6, 2021. https://www.plannedparenthood.org/learn/abortion/the-abortion-pill
