

Association of Tourette Syndrome and Chronic Tic Disorder With Violent Assault and Criminal Convictions
- PMID: 35311941
- PMCID: PMC8938899
- DOI: 10.1001/jamaneurol.2022.0167
Association of Tourette Syndrome and Chronic Tic Disorder With Violent Assault and Criminal Convictions
Abstract
Importance: Tic disorders are associated with multiple social adversities, but little is known about the experience of violent assault (including sexual assault) and criminality in this group.
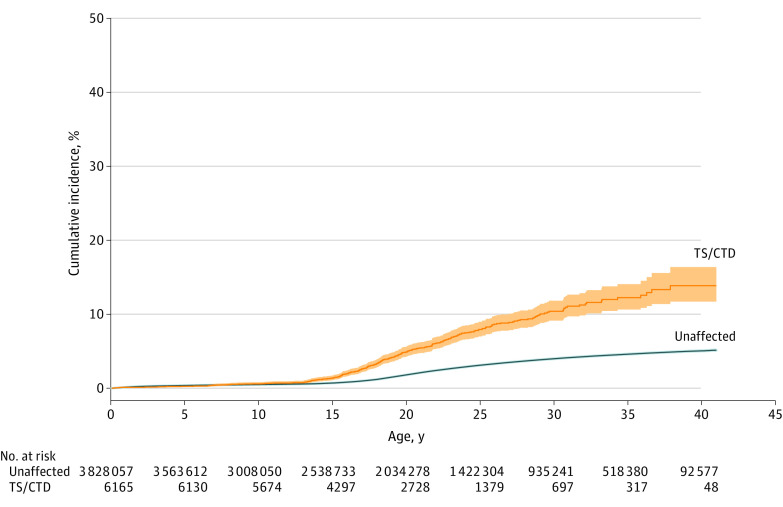
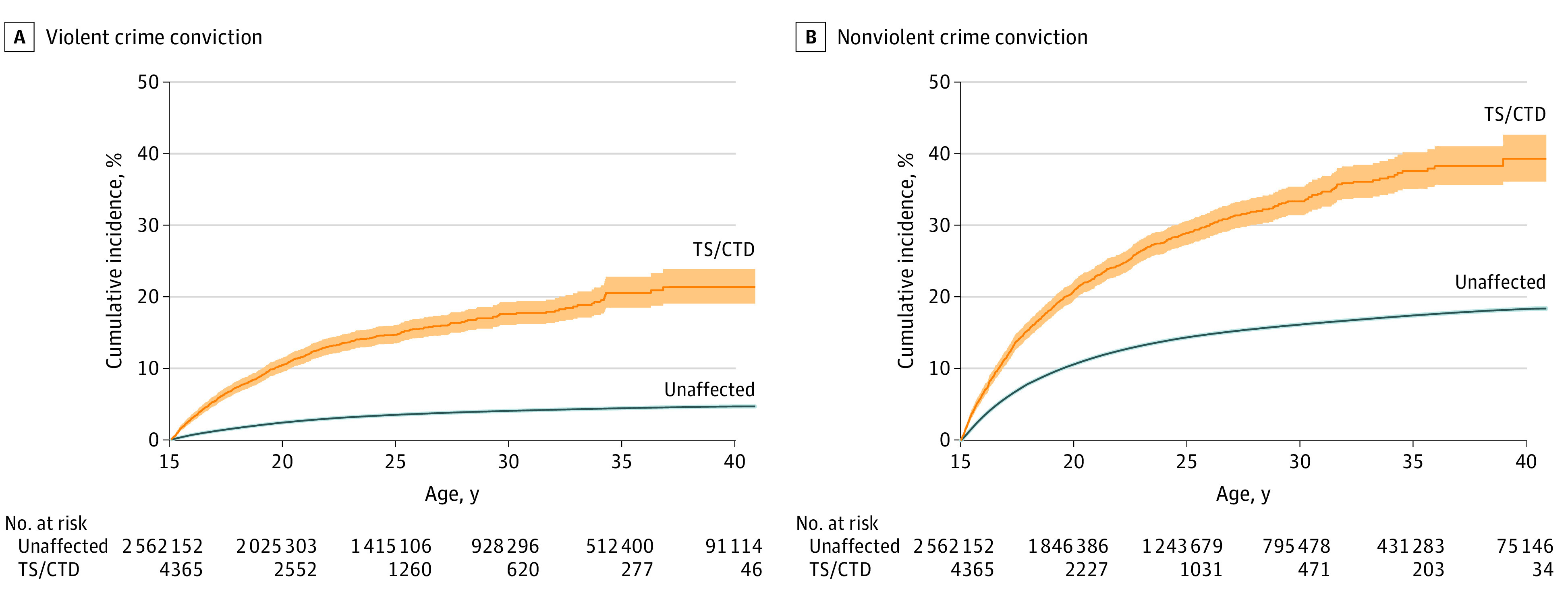
Objective: To establish if Tourette syndrome (TS) and chronic tic disorder (CTD) are associated with an increased risk of experiencing violent assault and criminal convictions.
Design, setting, and participants: In this cohort study, all individuals living in Sweden at any time between January 1, 1973, and December 31, 2013, were identified from Swedish nationwide health and administrative registers. Cox proportional hazards regression models were used to estimate the risk of violent assault and criminal convictions among people with TS or CTD, compared with the general population and unaffected full siblings. Data analyses were conducted between September 1 and October 22, 2021.
Exposures: The Swedish version of the International Classification of Diseases, Eighth Revision (ICD-8), ICD-9, and ICD-10 diagnoses of TS or CTD in the Swedish National Patient Register.
Main outcomes and measures: Records of sexual and nonsexual violent assault and death due to violent assaults were obtained from the National Patient Register and the Cause of Death Register, respectively. Convictions for violent and nonviolent criminal offenses were obtained from the Crime Register. Covariates included sex and birth year.
Results: The study cohort included 13 819 284 individuals living in Sweden between 1973 and 2013. A total of 7791 individuals with TS or CTD were identified (median [IQR] age at first diagnosis, 13.4 [10.0-21.8] years; 5944 [76%] male). Compared with unaffected individuals from the general population, people with TS or CTD had a 2-fold increased risk of experiencing any violent assault (sexual and nonsexual) (adjusted hazard ratio [aHR], 2.21; 95% CI, 2.00-2.43), a 3-fold increased risk of violent convictions (aHR, 3.13; 95% CI, 2.92-3.36), and a 1.6-fold increased risk of nonviolent crime convictions (aHR, 1.62; 95% CI, 1.54-1.71). Among people with TS or CTD, 37.0% (114 of 308; 95% CI, 31.6%-42.4%) of individuals who had experienced violent assault also had a violent crime conviction, compared with 17.9% (16 067 of 89 920; 95% CI, 17.6%-18.1%) in the general population. Exclusion of individuals with attention-deficit/hyperactivity disorder and substance use disorders partially attenuated the associations. Similarly, within-sibling models attenuated but did not eliminate the associations (any violent assault: aHR, 1.32; 95% CI, 1.08-1.61; violent crime: aHR, 2.23; 95% CI, 1.86-2.67; nonviolent crime: aHR, 1.34; 95% CI, 1.20-1.50).
Conclusions and relevance: Results of this cohort study suggest that most individuals with TS or CTD are not assaulted nor are perpetrators of crime. However, individuals with TS or CTD diagnosed in specialist settings were more likely to both experience violent assault and be perpetrators of violence compared with the general population. The risk was highest in individuals with comorbid attention-deficit/hyperactivity disorder and substance use disorders. The increased risk found in specialty clinics will need to be better understood in the general population.
Conflict of interest statement
Figures
Comment in
-
Why Some Individuals With Tourette Syndrome Experience Assault and Perpetrate Criminal Behavior.JAMA Neurol. 2022 May 1;79(5):442-444. doi: 10.1001/jamaneurol.2021.5541. JAMA Neurol. 2022. PMID: 35311951 No abstract available.
References
-
- Hirschtritt ME, Lee PC, Pauls DL, et al. ; Tourette Syndrome Association International Consortium for Genetics . Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry. 2015;72(4):325-333. doi: 10.1001/jamapsychiatry.2014.2650 - DOI - PMC - PubMed
-
- Pérez-Vigil A, Fernández de la Cruz L, Brander G, et al. Association of Tourette syndrome and chronic tic disorders with objective indicators of educational attainment: a population-based sibling comparison study. JAMA Neurol. 2018;75(9):1098-1105. doi: 10.1001/jamaneurol.2018.1194 - DOI - PMC - PubMed
