

Evaluation of ocular biometry in primary angle-closure disease with two swept source optical coherence tomography devices
- PMID: 35312733
- PMCID: PMC8936461
- DOI: 10.1371/journal.pone.0265844
Evaluation of ocular biometry in primary angle-closure disease with two swept source optical coherence tomography devices
Abstract
Purpose: To investigate agreement between 2 swept source OCT biometers, IOL Master700 and Anterion, in various ocular biometry and intraocular lens (IOL) calculations of primary angle-closure disease (PACD).
Setting: Rajavithi Hospital, Bangkok, Thailand.
Design: Prospective comparative study.
Methods: This study conducted in a tertiary eye care center involving biometric measurements obtained with 2 devices in phakic eye with diagnosis of PACD. Mean difference and intraclass correlation coefficient (ICC) with confidence limits were assessed, and calculations of estimated residual refraction of the IOL were analysed using Barrett's formula.
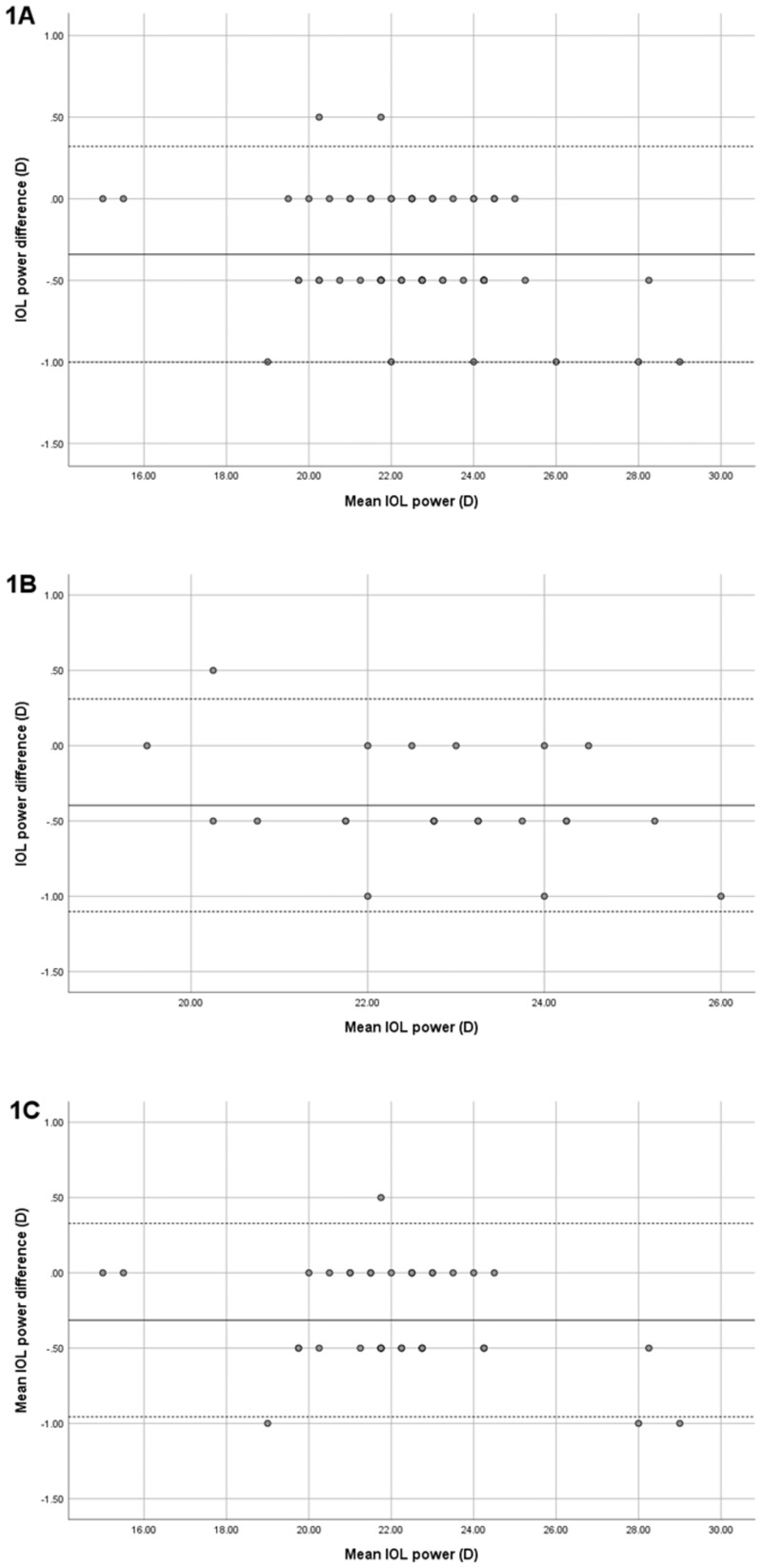
Results: Sixty-nine eyes from 45 PACD patients were enrolled for the study. Excellent agreement of various parameters was revealed, with ICC (confidence limits) of K1 = 0.953 (0.861-0.979), K2 = 0.950 (0.778-0.98), ACD = 0.932 (0.529-0.978), WTW = 0.775 (0.477-0.888), and LT = 0.947 (0.905-0.97). Mean difference of axial length (AL) was -0.01 ± 0.02 mm with ICC of 1.000. IOL calculation was assessed with Barrett's formula, and Bland-Altman plot showed excellent agreement in the results of the 2 devices for the IOL power and estimated post-operative residual refraction (EPR).
Conclusions: Mean differences of biometric parameters, obtained with IOL Master700 and Anterion, were small, and ICC showed excellent concordance. No clinical relevance in calculation of IOL power was found, and the two devices appeared to be comparably effective in clinical practice.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Gazzard G, Foster PJ, Viswanathan AC, Devereux JG, Oen FT, Chew PTK, et al. The severity and spatial distribution of visual field defects in primary glaucoma: a comparison of primary open-angle glaucoma and primary angle-closure glaucoma. Archives of Ophthalmology. 2002;120(12):1636–43. doi: 10.1001/archopht.120.12.1636 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
