

Integrating a physical activity coaching intervention into diabetes care: a mixed-methods evaluation of a pilot pragmatic trial
- PMID: 35312788
- PMCID: PMC9150080
- DOI: 10.1093/tbm/ibac014
Integrating a physical activity coaching intervention into diabetes care: a mixed-methods evaluation of a pilot pragmatic trial
Abstract
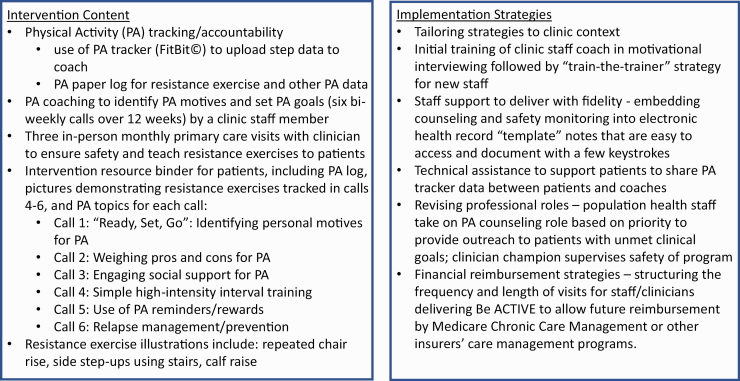
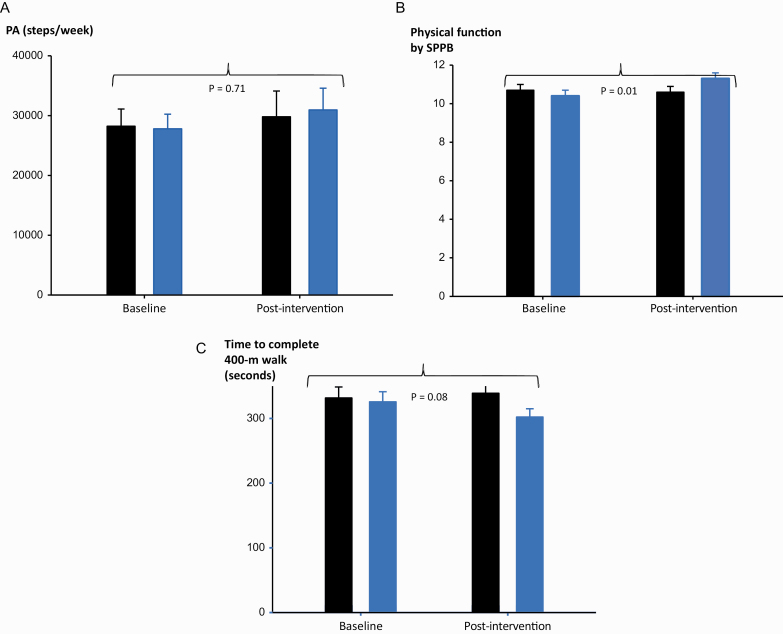
Physical activity (PA) counseling is under-utilized in primary care for patients with type 2 diabetes mellitus (T2D), despite improving important health outcomes, including physical function. We adapted evidence-based PA counseling programs to primary care patients, staff, and leader's needs, resulting in "Be ACTIVE" comprised of shared PA tracker data (FitBit©), six theory-informed PA coaching calls, and three in-person clinician visits. In a pilot randomized pragmatic trial, we evaluated the feasibility, acceptability, and effectiveness of Be ACTIVE. Sedentary patients with T2D were randomized to Be ACTIVE versus an enhanced control condition. Mixed methods assessments of feasibility and acceptability included costs. Objective pilot effectiveness outcomes included PA (primary outcome, accelerometer steps/week), the Short Physical Performance Battery (SPPB) physical function measure, and behavioral PA predictors. Fifty patients were randomized to Be ACTIVE or control condition. Acceptability was >90% for patients and clinic staff. Coaching and PA tracking costs of ~$90/patient met Medicare reimbursement criteria. Pre-post PA increased by ~11% (Be ACTIVE) and ~6% in controls (group difference: 1574 ± 4391 steps/week, p = .72). As compared to controls, Be ACTIVE participants significantly improved SPPB (0.9 ± 0.3 vs. -0.1 ± 0.3, p = .01, changes >0.5 points prevent falls clinically), and PA predictors of self-efficacy (p = .02) and social-environmental support (p < .01). In this pilot trial, Be ACTIVE was feasible and highly acceptable to stakeholders and yielded significant improvements in objective physical function consistent with lower fall risk, whereas PA changes were less than anticipated. Be ACTIVE may need additional adaptation or a longer duration to improve PA outcomes.
Trial registration: ClinicalTrials.gov NCT02473926.
Keywords: Implementation; Physical activity; Physical function; Primary care; Type 2 diabetes mellitus; acceptability.
Plain language summary
We report results from a pragmatic and behavioral theory-based physical activity (PA) coaching program, termed “Be ACTIVE,” for patients with type 2 diabetes that was designed to improve PA and function for patients and to be reimbursable and feasible for primary care teams. As compared to those who did not receive coaching, patients who received Be ACTIVE had physical function improvements that lowered their risk of falls. Be ACTIVE was delivered with fidelity and was highly acceptable to the key primary care stakeholders of patients, clinic staff coaches, and clinicians. Patients particularly liked the focus on setting goals to do enjoyable activities, the accountability of wearing a PA monitor, and the support of their coach. Clinical care professionals felt that their role of encouraging behavior change (coach) and safety monitoring (clinician) aligned well with their clinical expertise, and was professionally rewarding. Coaches felt the program helped them guide many patients to overcome preexisting negative perceptions of PA and develop intrinsic motivations to be active. The costs of clinic coach time and PA tracker rental needed to deliver the 12-week program could be reimbursed by the Medicare Chronic Disease Management programs, albeit with a patient co-payment required.
© Society of Behavioral Medicine 2022. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Feasibility and Cultural Adaptation of a Community-Engaged Physical Activity Intervention for Hispanic Older Adults: Pilot Study.JMIR Form Res. 2025 May 27;9:e65489. doi: 10.2196/65489. JMIR Form Res. 2025. PMID: 40424571 Free PMC article.
-
Piloting HealthScore: Feasibility and acceptability of a clinically integrated health coaching program for people living with cancer.Cancer Med. 2023 Apr;12(7):8804-8814. doi: 10.1002/cam4.5625. Epub 2023 Jan 16. Cancer Med. 2023. PMID: 36647557 Free PMC article.
-
The Feasibility of the Diabetes Self-Management Coaching Program in Primary Care: A Mixed-Methods Randomized Controlled Feasibility Trial.Int J Environ Res Public Health. 2024 Aug 6;21(8):1032. doi: 10.3390/ijerph21081032. Int J Environ Res Public Health. 2024. PMID: 39200642 Free PMC article. Clinical Trial.
-
Health Coaching and Its Impact in the Remote Management of Patients With Type 2 Diabetes Mellitus: Scoping Review of the Literature.J Med Internet Res. 2025 Apr 9;27:e60703. doi: 10.2196/60703. J Med Internet Res. 2025. PMID: 40202791 Free PMC article.
-
Demystifying diabetes health coaching: A scoping review unveiling the 'who' and 'where' of health coaching for adults with type 2 diabetes.Diabet Med. 2024 Jun;41(6):e15327. doi: 10.1111/dme.15327. Epub 2024 Apr 10. Diabet Med. 2024. PMID: 38597813
Cited by
-
A narrative review of exercise participation among adults with prediabetes or type 2 diabetes: barriers and solutions.Front Clin Diabetes Healthc. 2023 Aug 30;4:1218692. doi: 10.3389/fcdhc.2023.1218692. eCollection 2023. Front Clin Diabetes Healthc. 2023. PMID: 37711232 Free PMC article. Review.
-
Type 2 diabetes is linked to higher physiologic markers of effort during exercise.Front Clin Diabetes Healthc. 2024 Apr 29;5:1346716. doi: 10.3389/fcdhc.2024.1346716. eCollection 2024. Front Clin Diabetes Healthc. 2024. PMID: 38741611 Free PMC article.
-
Pragmatic considerations and approaches for measuring staff time as an implementation cost in health systems and clinics: key issues and applied examples.Implement Sci Commun. 2022 Apr 15;3(1):44. doi: 10.1186/s43058-022-00292-4. Implement Sci Commun. 2022. PMID: 35428326 Free PMC article.
-
MOMs Chat & Care Study: Rationale and design of a pragmatic randomized clinical trial to prevent severe maternal morbidity among Black birthing people.Contemp Clin Trials. 2025 May;152:107850. doi: 10.1016/j.cct.2025.107850. Epub 2025 Feb 21. Contemp Clin Trials. 2025. PMID: 39987957
-
Implementation determinants of physical activity interventions in primary health care settings using the TICD framework: a systematic review.BMC Health Serv Res. 2023 Oct 11;23(1):1082. doi: 10.1186/s12913-023-09881-y. BMC Health Serv Res. 2023. PMID: 37821932 Free PMC article.
References
-
- Zhao G, Ford ES, Li C, Balluz LS. Physical activity in U.S. older adults with diabetes mellitus: Prevalence and correlates of meeting physical activity recommendations. J Am Geriatr Soc. 2011;59(1):132–137. - PubMed
-
- Gregg EW, Menke A. Diabetes and disability. In: Diabetes in America, 3rd ed., National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). 2018:34.31–34.15. https://www.niddk.nih.gov/about-niddk/strategic-plans-reports/diabetes-i....
-
- Kirk A, Mutrie N, MacIntyre P, Fisher M. Effects of a 12-month physical activity counselling intervention on glycaemic control and on the status of cardiovascular risk factors in people with Type 2 diabetes. Diabetologia. 2004;47(5):821–832. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
