

Precision dosimetry in yttrium-90 radioembolization through CT imaging of radiopaque microspheres in a rabbit liver model
- PMID: 35312882
- PMCID: PMC8938593
- DOI: 10.1186/s40658-022-00447-1
Precision dosimetry in yttrium-90 radioembolization through CT imaging of radiopaque microspheres in a rabbit liver model
Erratum in
-
Correction: Precision dosimetry in yttrium-90 radioembolization through CT imaging of radiopaque microspheres in a rabbit liver model.EJNMMI Phys. 2023 Nov 29;10(1):74. doi: 10.1186/s40658-023-00596-x. EJNMMI Phys. 2023. PMID: 38017227 Free PMC article. No abstract available.
Abstract
Purpose: To perform precision dosimetry in yttrium-90 radioembolization through CT imaging of radiopaque microspheres in a rabbit liver model and to compare extracted dose metrics to those produced from conventional PET-based dosimetry.
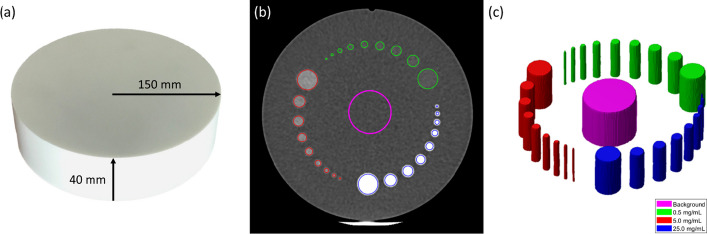
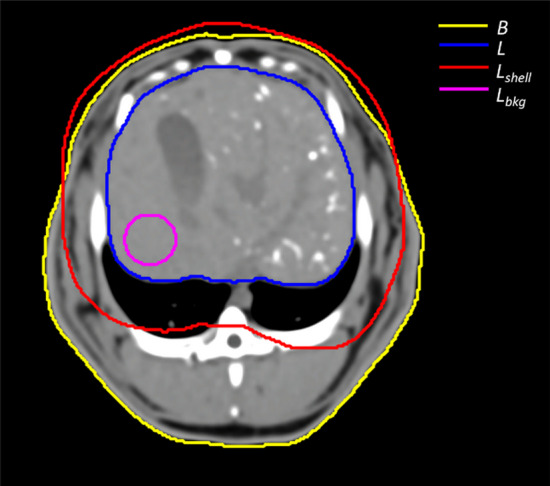
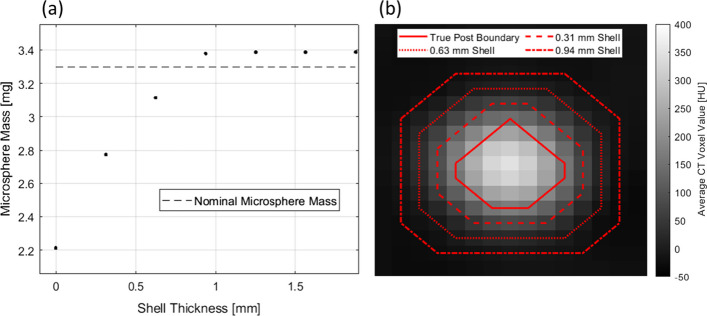
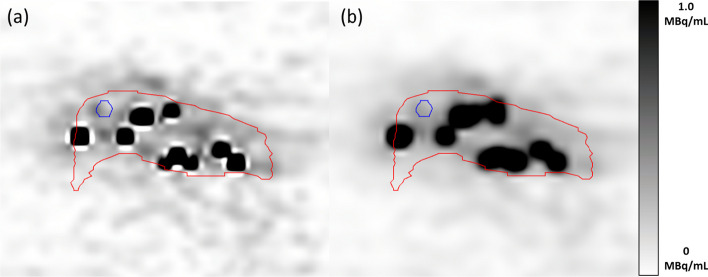
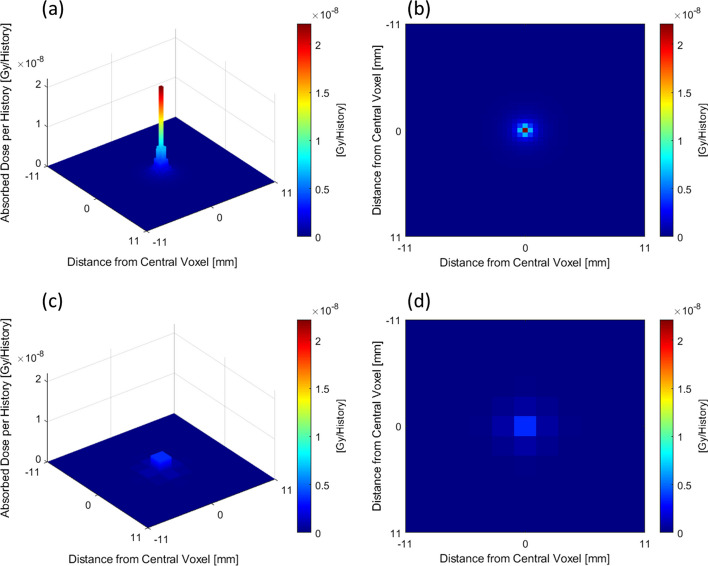
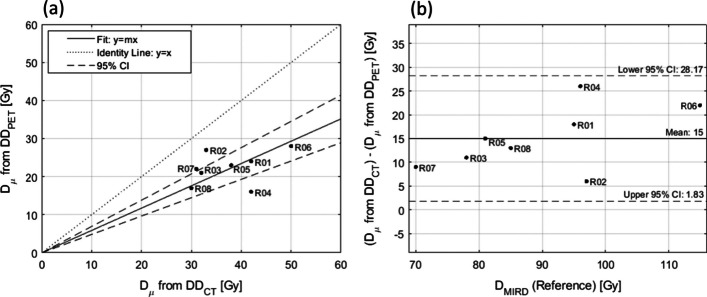
Materials and methods: A CT calibration phantom was designed containing posts with nominal microsphere concentrations of 0.5 mg/mL, 5.0 mg/mL, and 25.0 mg/mL. The mean Hounsfield unit was extracted from the post volumes to generate a calibration curve to relate Hounsfield units to microsphere concentration. A nominal bolus of 40 mg of microspheres was administered to the livers of eight rabbits, followed by PET/CT imaging. A CT-based activity distribution was calculated through the application of the calibration curve to the CT liver volume. Post-treatment dosimetry was performed through the convolution of yttrium-90 dose-voxel kernels and the PET- and CT-based cumulated activity distributions. The mean dose to the liver in PET- and CT-based dose distributions was compared through linear regression, ANOVA, and Bland-Altman analysis.
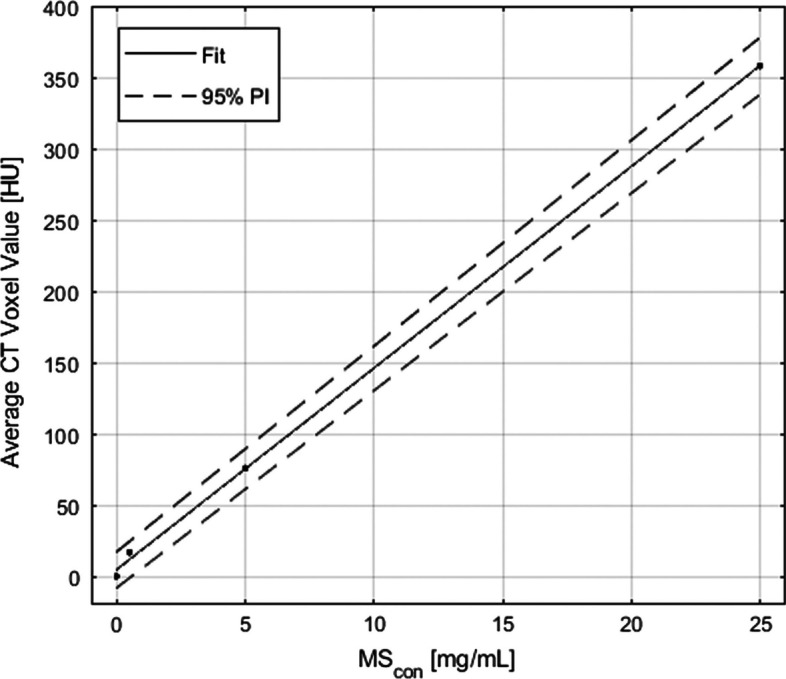
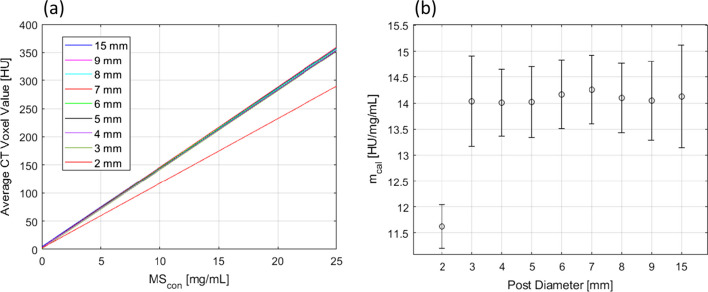
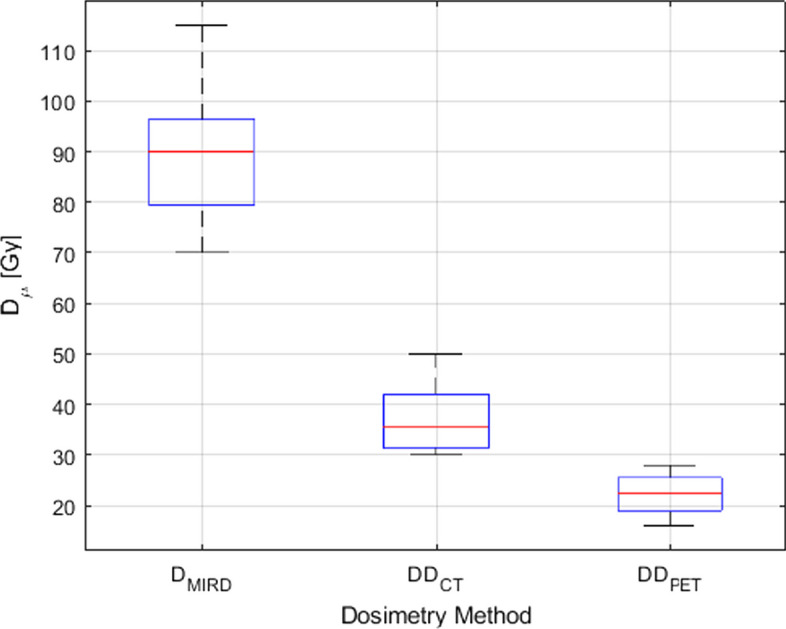
Results: A linear least-squares fit to the average Hounsfield unit and microsphere concentration data from the calibration phantom confirmed a strong correlation (r2 > 0.999) with a slope of 14.13 HU/mg/mL. A poor correlation was found between the mean dose derived from CT and PET (r2 = 0.374), while the ANOVA analysis revealed statistically significant differences (p < 10-12) between the MIRD-derived mean dose and the PET- and CT-derived mean dose. Bland-Altman analysis predicted an offset of 15.0 Gy between the mean dose in CT and PET. The dose within the liver was shown to be more heterogeneous in CT than in PET with an average coefficient of variation equal to 1.99 and 1.02, respectively.
Conclusion: The benefits of a CT-based approach to post-treatment dosimetry in yttrium-90 radioembolization include improved visualization of the dose distribution, reduced partial volume effects, a better representation of dose heterogeneity, and the mitigation of respiratory motion effects. Post-treatment CT imaging of radiopaque microspheres in yttrium-90 radioembolization provides the means to perform precision dosimetry and extract accurate dose metrics used to refine the understanding of the dose-response relationship, which could ultimately improve future patient outcomes.
Keywords: CT; Dosimetry; Microsphere; PET; Radioembolization; Radiopacity; Yttrium-90.
© 2022. The Author(s).
Conflict of interest statement
RA is a shareholder, cofounder, and Chief Medical Officer of ABK Biomedical. AS, ECH, ACG, and DL have provided consulting services to ABK Biomedical. JNB has received research support from ABK Biomedical. SCK has received research support from and served as a consultant for Boston Scientific, Sirtex Medical, and ABK Biomedical. DL has received research support from Boston Scientific and served as a consultant for Sirtex Medical and ABK Biomedical.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources
