

Analgesic Efficacy of Transverse Abdominis Plane Block and Quadratus Lumborum Block in Laparoscopic Sleeve Gastrectomy: A Randomized Double-Blinded Clinical Trial
- PMID: 35312948
- PMCID: PMC9098772
- DOI: 10.1007/s40122-022-00373-1
Analgesic Efficacy of Transverse Abdominis Plane Block and Quadratus Lumborum Block in Laparoscopic Sleeve Gastrectomy: A Randomized Double-Blinded Clinical Trial
Abstract
Introduction: The analgesic effect and safety of transversus abdominis plane block (TAPB) is still controversial in various abdominal procedures. Quadratus lumborum block (QLB) has been considered to provide a widespread and long-lasting analgesic effect in gynecological surgeries. However, the analgesic effects of these two techniques in patients with extreme obesity undergoing laparoscopic sleeve gastrectomy (LSG) are still unknown.
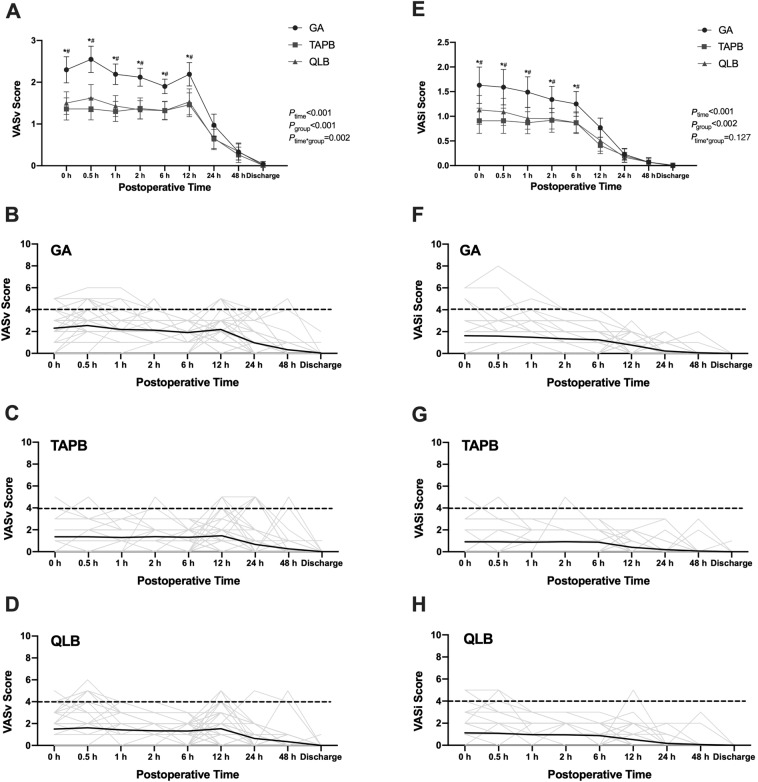
Methods: A total of 225 patients with obesity were randomly assigned to group TAPB (n = 76, 30 ml 0.33% ropivacaine with dexmedetomidine 1 μg kg-1), group QLB (n = 76, 30 ml 0.33% ropivacaine with dexmedetomidine 1 μg kg-1), or general anesthesia alone (GA, n = 73, 30 ml 0.9% saline). During the 48-h postoperative period, patients received continuous intravenous patient-controlled analgesia (PCA) containing sufentanil 2 μg kg-1, dexmedetomidine 2 μg kg-1, and granisetron 3 mg. The scores of visual analogue scale (VAS) in surgical incision and viscera, considering as the primary outcomes, were continuously recorded at postoperative 0, 0.5, 1, 2, 6, 12, 24, 48 h and discharge.
Results: Comparing with patients in the GA group, VAS scores of incision and viscera were consistently reduced during the initial 6-12 h after LSG in TAPB and QLB groups, and they received less propofol and remifentanil (P < 0.001) as well. In the QLB group, patients had longer duration for the first rescue analgesia, and fewer requirements of the rescue analgesia within 24 h than the GA group (P < 0.05). In addition, there were fewer PCA requirements in QLB group than GA and TAPB groups (P < 0.05).
Conclusions: Ultrasound-guided transversus abdominis plane block and quadratus lumborum block could provide comparable analgesic effects for a laparoscopic sleeve gastrectomy in obese patients.
Trial registration: Chinese Clinical Trial Registry; ChiCTR1800019236.
Keywords: Laparoscopic sleeve gastrectomy; Obesity; Postoperative pain; Quadratus lumbar nerve block; Transversus abdominis plane block.
© 2022. The Author(s).
Figures

References
-
- Pöpping DM, Zahn PK, Van Aken HK, et al. Effectiveness and safety of postoperative pain management: a survey of 18,925 consecutive patients between 1998 and 2006 (2nd revision): a database analysis of prospectively raised data. Br J Anaesth. 2008;101(6):832–840. doi: 10.1093/bja/aen300. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
