

Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Nasal Cavity, Paranasal Sinuses and Skull Base
- PMID: 35312976
- PMCID: PMC9018924
- DOI: 10.1007/s12105-021-01406-5
Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Nasal Cavity, Paranasal Sinuses and Skull Base
Abstract
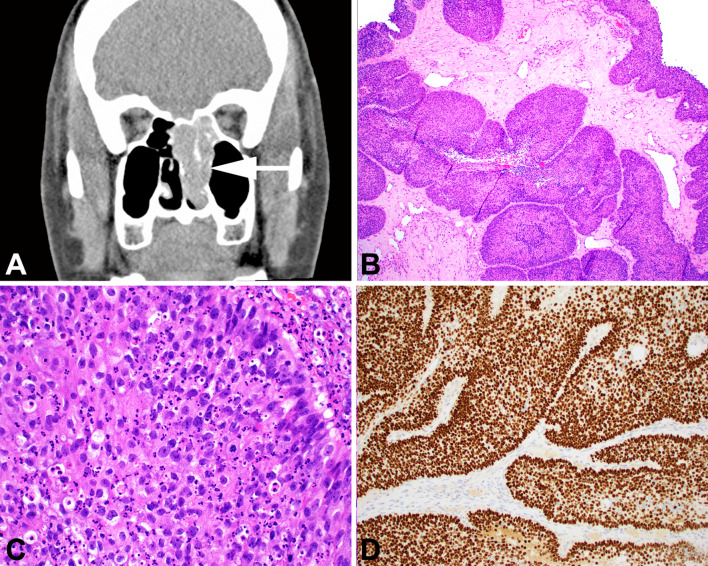
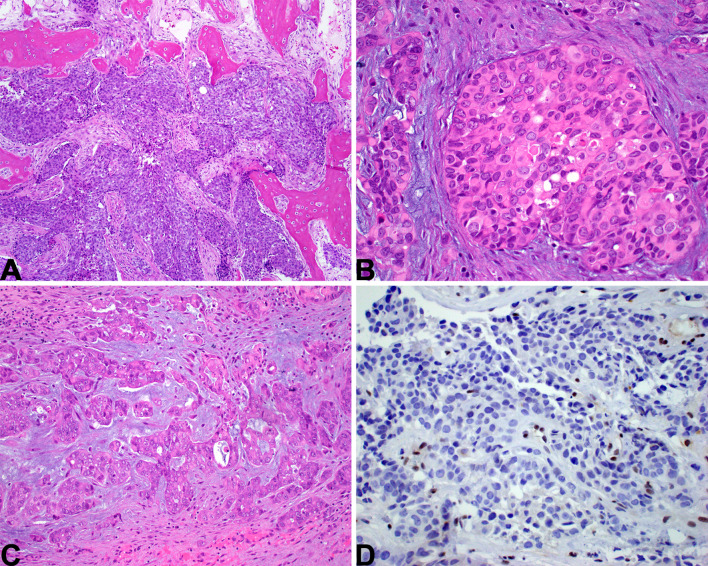
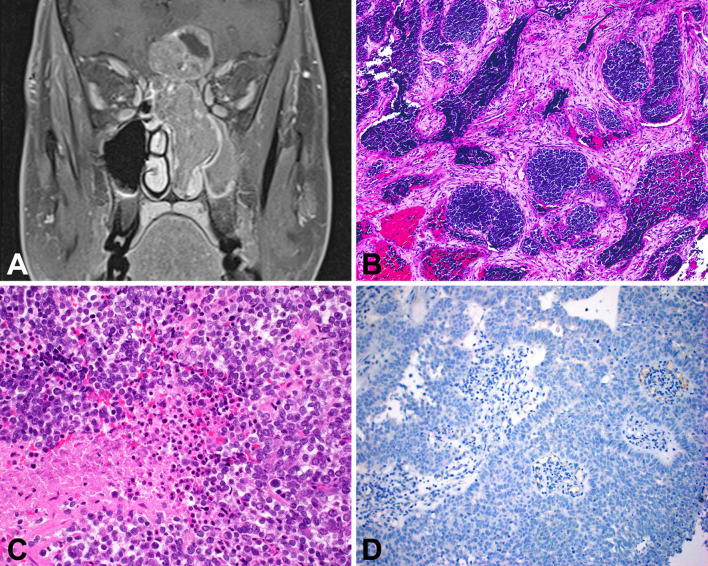
The World Health Organization Classification of Head and Neck Tumours recently published the 5th edition. There are new entities, emerging entities, and significant updates to the taxonomy and characterization of tumor and tumor-like lesions, specifically in this article as it relates to nasal cavity, paranasal sinuses and skull base. Importantly, the number of diagnostic entries has been reduced by creating category-specific chapters for soft tissue, hematolymphoid, melanocytic, neuroectodermal, and metastatic tumors. Bone and salivary gland tumors are also not separately reported in the sinonasal tract, but included in the jaw and salivary gland sections, respectively. Repetition of characteristic entities in each anatomic site was also reduced, instead highlighting only the unique features in each anatomic site. Two new entities (SWI/SNF complex-deficient sinonasal carcinomas and HPV-related multiphenotypic sinonasal carcinoma) will be highlighted in this review, with a discussion of several emerging entities. There is a short description of updated information for all 24 diagnostic entities included in this edition to allow the reader a snapshot of current state of knowledge, but to encourage more investigation and further broaden understanding of these diverse and rare entities.
Keywords: Carcinoma; Immunohistochemistry; Nasal cavity; Papillomavirus neoplasms; Paranasal sinus neoplasms; Paranasal sinuses; SWI/SNF complex; Skull base; World Health Organization.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
All authors have contributed to this work and both authors declare they have no conflict of interest as it relates to this study.
Figures
References
-
- Bishop JA, Loney EL, Thompson LDR. Nasal cavity, paranasal sinuses, and skull base tumours. In: Board WCTE, editor. Head and neck tumours. 5. Lyon: International Agency for Research on Cancer; 2022.
-
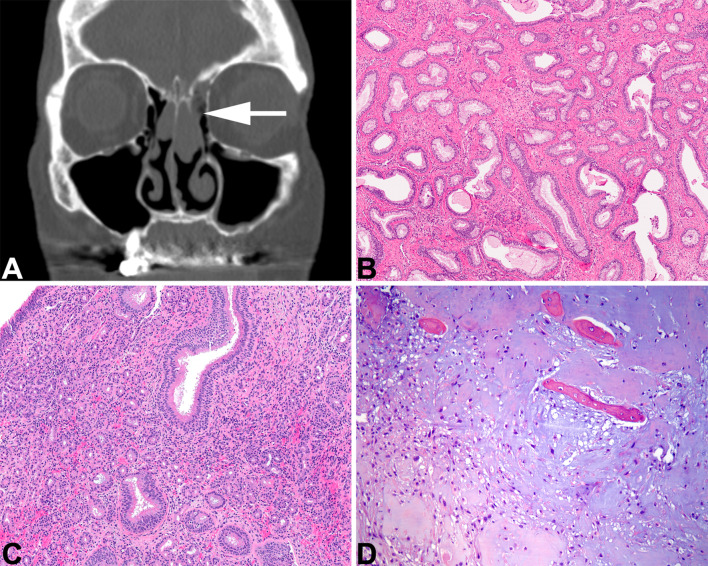
- Ozolek JA, Hunt JL. Tumor suppressor gene alterations in respiratory epithelial adenomatoid hamartoma (REAH): comparison to sinonasal adenocarcinoma and inflamed sinonasal mucosa. Am J Surg Pathol. 2006;30:1576–1580. - PubMed
-
- Baneckova M, Michal M, Laco J, et al. Immunohistochemical and genetic analysis of respiratory epithelial adenomatoid hamartomas and seromucinous hamartomas: are they precursor lesions to sinonasal low-grade tubulopapillary adenocarcinomas? Hum Pathol. 2020;97:94–102. - PubMed
-
- Lee JT, Garg R, Brunworth J, Keschner DB, Thompson LD. Sinonasal respiratory epithelial adenomatoid hamartomas: series of 51 cases and literature review. Am J Rhinol Allergy. 2013;27:322–328. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
