

Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Salivary Glands
- PMID: 35312980
- PMCID: PMC9018948
- DOI: 10.1007/s12105-022-01420-1
Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Salivary Glands
Abstract
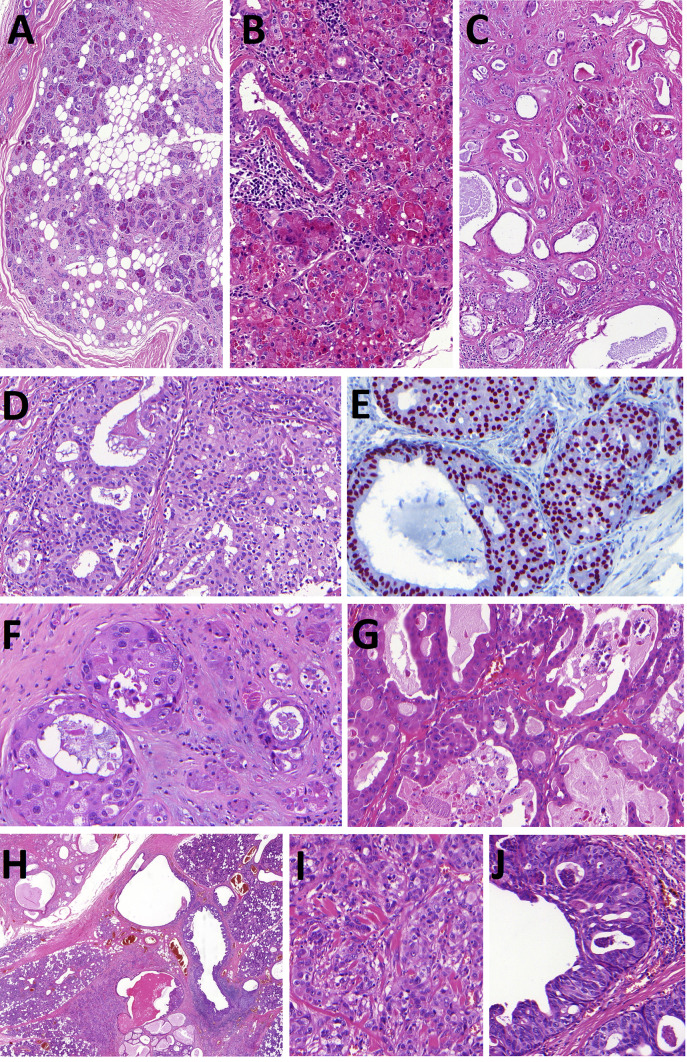
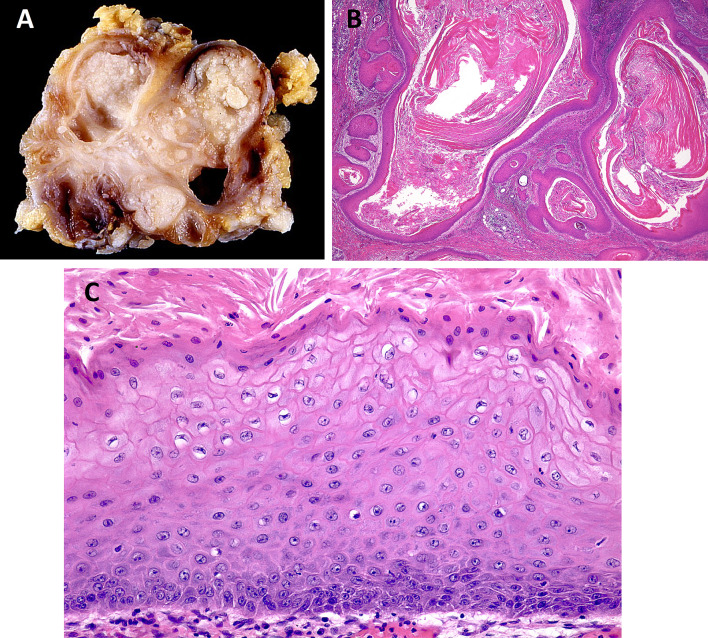
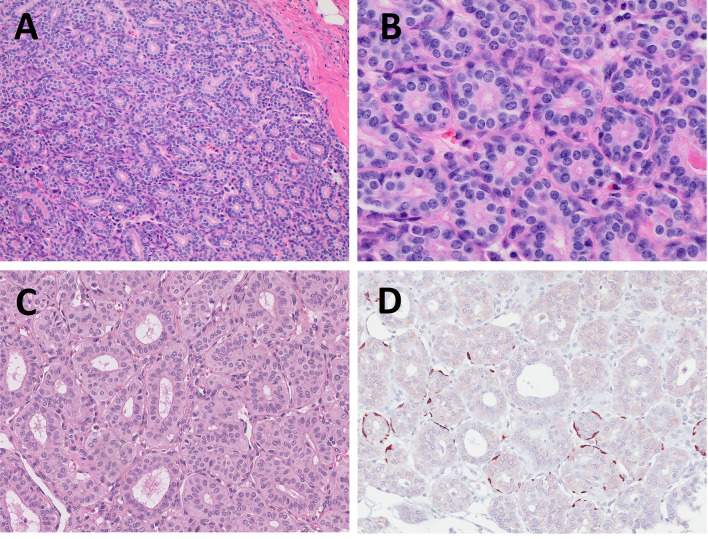
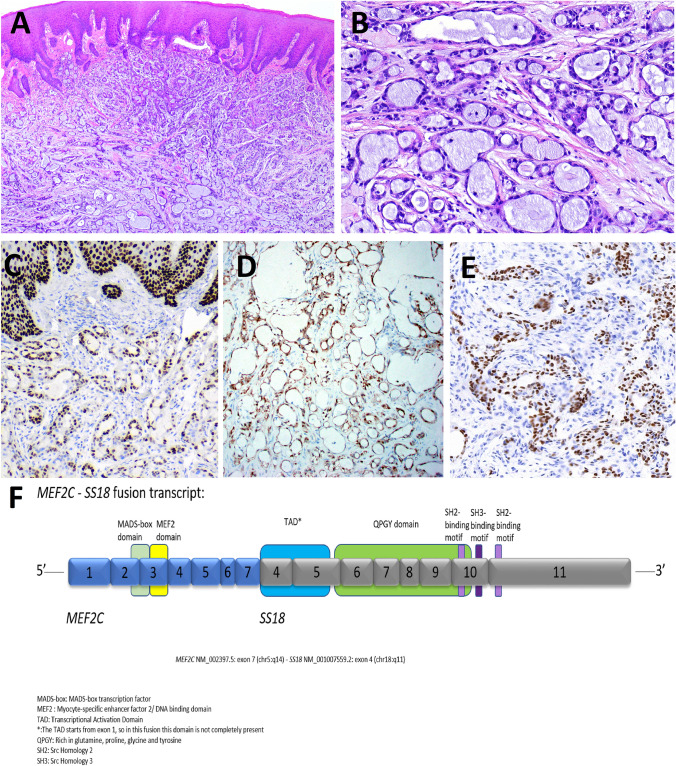
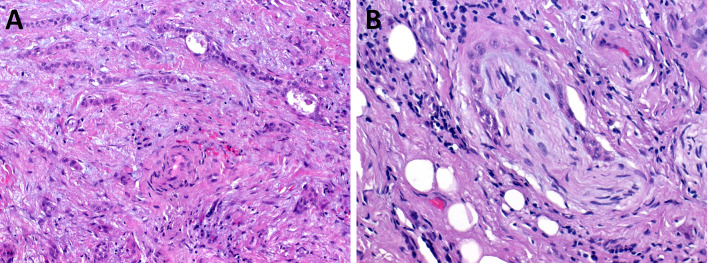
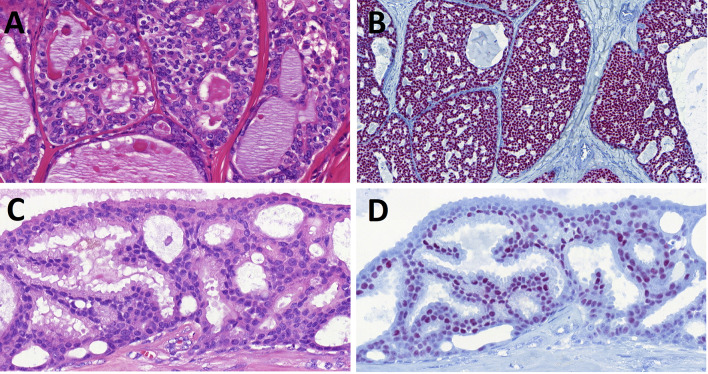
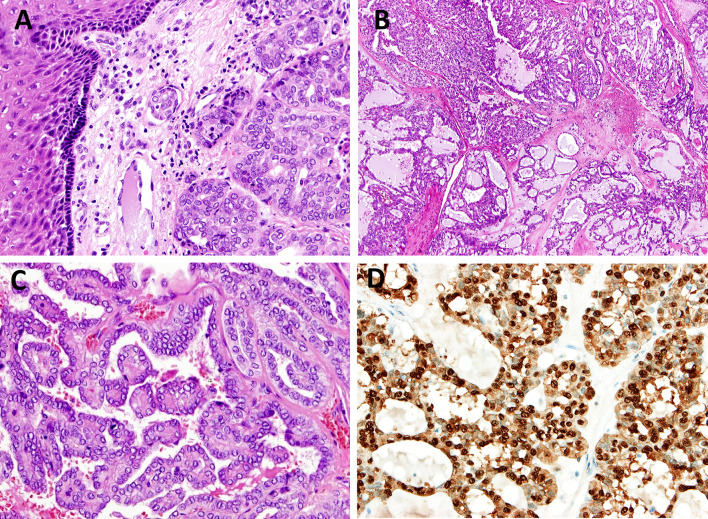
The salivary gland section in the 5th edition of the World Health Organization Classification of Head and Neck Tumours features a description and inclusion of several new entities, including sclerosing polycystic adenoma, keratocystoma, intercalated duct adenoma, and striated duct adenoma among the benign neoplasms; and microsecretory adenocarcinoma and sclerosing microcystic adenocarcinoma as the new malignant entities. The new entry also includes mucinous adenocarcinoma subdivided into papillary, colloid, signet ring, and mixed subtypes with recurrent AKT1 E17K mutations across patterns suggesting that mucin-producing salivary adenocarcinomas represent a histologically diverse single entity that may be related to salivary intraductal papillary mucinous neoplasm (IPMN). Importantly, the number of entities in the salivary chapter has been reduced by omitting tumors or lesions if they do not occur exclusively or predominantly in salivary glands, including hemangioma, lipoma, nodular fasciitis and hematolymphoid tumors. They are now discussed in detail elsewhere in the book. Cribriform adenocarcinoma of salivary gland origin (CASG) now represents a distinctive subtype of polymorphous adenocarcinoma (PAC). PAC is defined as a clinically, histologically and molecularly heterogeneous disease group. Whether CASG is a different diagnostic category or a variant of PAC is still controversial. Poorly differentiated carcinomas and oncocytic carcinomas are discussed in the category "Salivary carcinoma not otherwise specified (NOS) and emerging entities". New defining genomic alterations have been characterized in many salivary gland tumors. In particular, they include gene fusions, which have shown to be tightly tumor-type specific, and thus valuable for use in diagnostically challenging cases. The recurrent molecular alterations were included in the definition of mucoepidermoid carcinoma, adenoid cystic carcinoma, secretory carcinoma, polymorphous adenocarcinoma, hyalinizing clear cell carcinoma, mucinous adenocarcinoma, and microsecretory adenocarcinoma.
Keywords: Classification; Gene fusion; Neoplasm; Salivary gland; WHO; World Health Organization.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO Classification of Tumours Editorial Board. Head and neck tumours. Lyon (France): International Agency for Research on Cancer; 2022. (WHO classification of tumours series, 5th ed.; vol. 9). https://publications.iarc.fr/
-
- World Health Organisation classification of head and neck tumours. In: El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg P, editors. Tumours of the salivary glands. 4th edition. Lyon IARC press, 2017; 159–202 [Chapter 7].
-
- Skálová A, Stenman G, Simpson RHW, Hellquist H, Slouka D, Svoboda T, et al. The role of molecular testing in the differential diagnosis of salivary gland carcinomas. Am J Surg Pathol. 2018;42(2):e11–e27. - PubMed
-
- Toper MH, Sarioglu S. Molecular pathology of salivary gland neoplasms: diagnostic, prognostic, and predictive perspective. Adv Anat Pathol. 2021;28(2):81–93. - PubMed
-
- Faquin WC and Rossi ED, editors. Milan system for reporting salivary gland cytopathology. Springer International Publishing; 2018.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
