

Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Tumours of the Oral Cavity and Mobile Tongue
- PMID: 35312982
- PMCID: PMC9018914
- DOI: 10.1007/s12105-021-01402-9
Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Tumours of the Oral Cavity and Mobile Tongue
Abstract
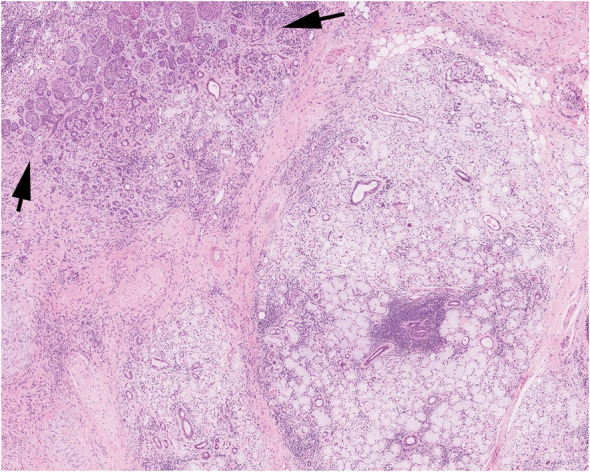
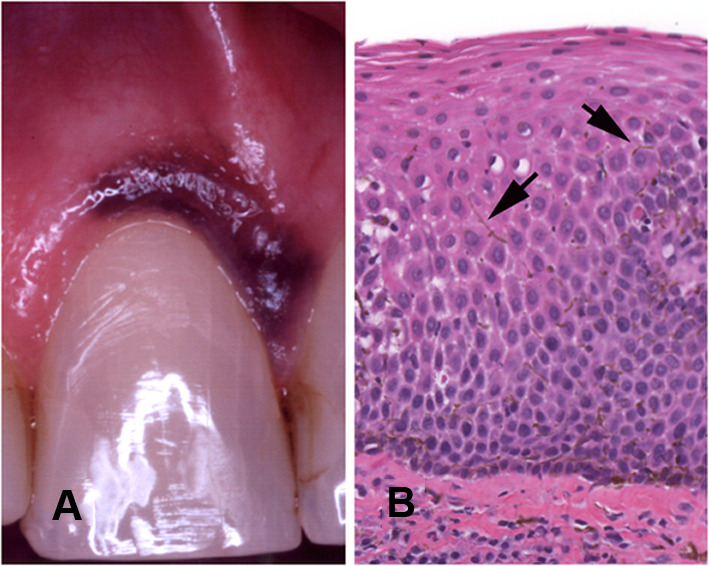
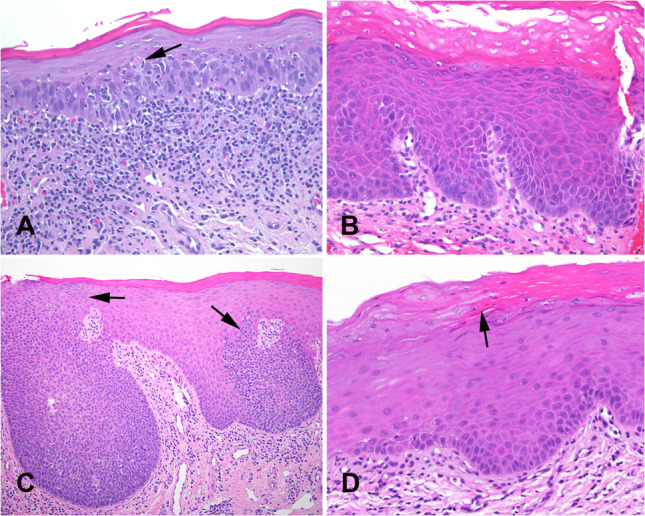
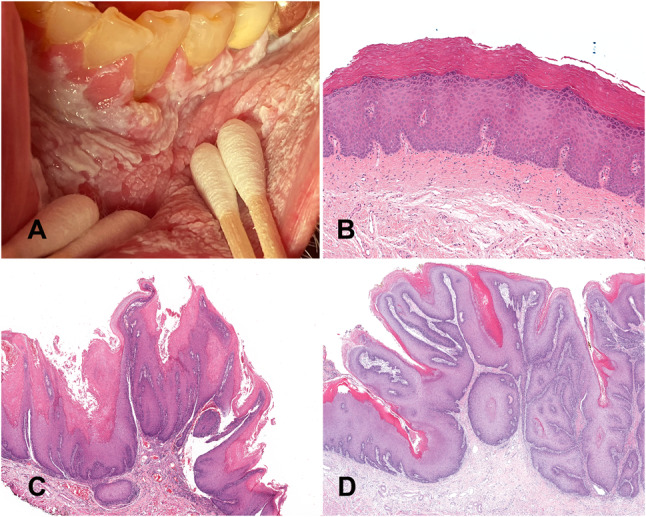
The fifth chapter of the upcoming fifth edition of the 2022 World Health Organization Classification of Tumours of the Head and Neck titled Tumours of the oral cavity and mobile tongue, has had some modifications from the 2017 fourth edition. A new section "Non-neoplastic Lesions", introduces two new entries: necrotizing sialometaplasia and melanoacanthoma. The combined Oral potentially malignant disorders and Oral epithelial dysplasia section in the 2015 WHO has now been separated and submucous fibrosis and HPV-associated dysplasia are also discussed in separate sections. Carcinoma cuniculatum and verrucous carcinoma are described in dedicated sections, reflecting that the oral cavity is the most common location in the head and neck for both these entities which have distinct clinical and histologic features from conventional squamous cell carcinoma. This review summarizes the changes in Chapter 5 with special reference to new additions, deletions, and sections that reflect current clinical, histological, and molecular advances.
Keywords: Dysplasia; Ectomesenchymal chondromyxoid tumor; Mobile tongue; Oral cavity; Proliferative verrucous leukoplakia; Squamous cell; Submucous fibrosis; World Health Organization.
© 2021. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Neither author has any conflicts of interest to disclose.
Figures
References
-
- WHO Classification of Tumours Editorial Board. Head and neck tumours (WHO classification of tumours series, 5th ed. vol. 9). Lyon (France): International Agency for Research on Cancer 2022.
-
- Carlson DL. Necrotizing sialometaplasia: a practical approach to the diagnosis. Arch Pathol Lab Med. 2009;133(5):692–698. - PubMed
-
- Abrams AM, Melrose RJ, Howell FV. Necrotizing sialometaplasia. A disease simulating malignancy. Cancer. 1973;32(1):130–135. - PubMed
-
- Fowler CB, Brannon RB. Subacute necrotizing sialadenitis: report of 7 cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89(5):600–609. - PubMed
-
- Kaplan I, et al. The clinical, histologic, and treatment spectrum in necrotizing sialometaplasia. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(5):577–585. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
