

Naming-related spectral responses predict neuropsychological outcome after epilepsy surgery
- PMID: 35313351
- PMCID: PMC9014727
- DOI: 10.1093/brain/awab318
Naming-related spectral responses predict neuropsychological outcome after epilepsy surgery
Abstract
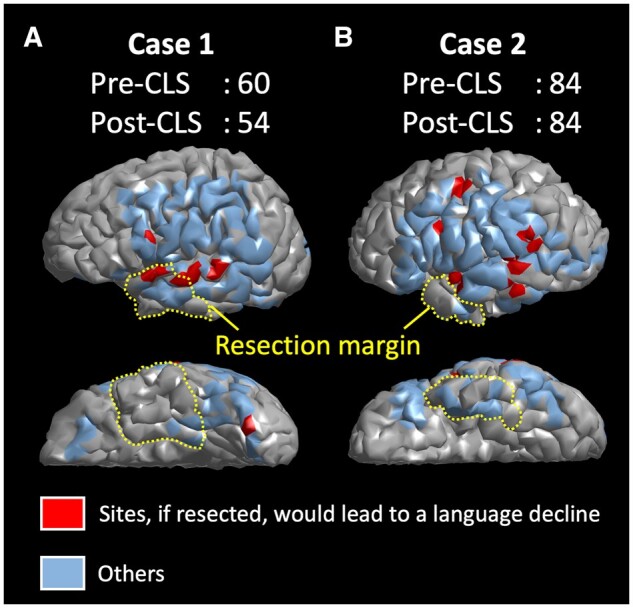
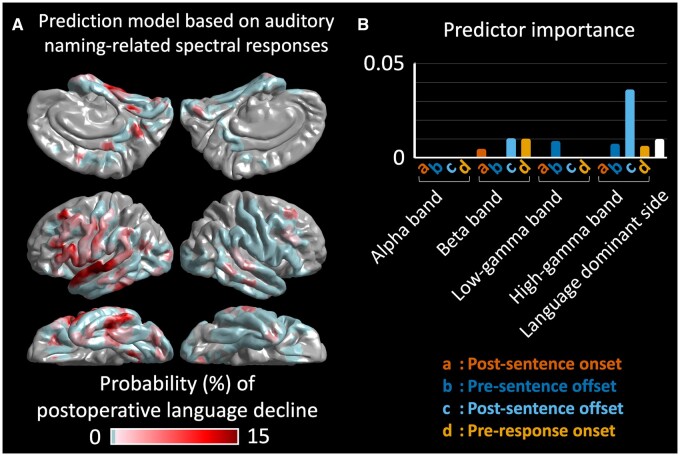
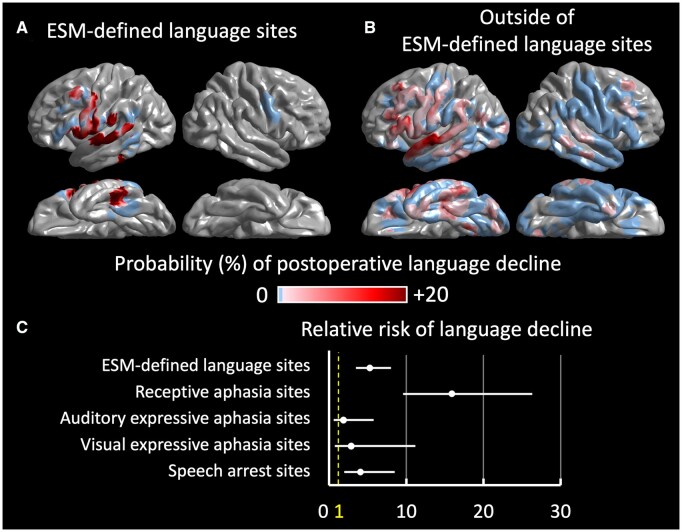
This prospective study determined the use of intracranially recorded spectral responses during naming tasks in predicting neuropsychological performance following epilepsy surgery. We recruited 65 patients with drug-resistant focal epilepsy who underwent preoperative neuropsychological assessment and intracranial EEG recording. The Clinical Evaluation of Language Fundamentals evaluated the baseline and postoperative language function. During extra-operative intracranial EEG recording, we assigned patients to undergo auditory and picture naming tasks. Time-frequency analysis determined the spatiotemporal characteristics of naming-related amplitude modulations, including high gamma augmentation at 70-110 Hz. We surgically removed the presumed epileptogenic zone based on the intracranial EEG and MRI abnormalities while maximally preserving the eloquent areas defined by electrical stimulation mapping. The multivariate regression model incorporating auditory naming-related high gamma augmentation predicted the postoperative changes in Core Language Score with r2 of 0.37 and in Expressive Language Index with r2 of 0.32. Independently of the effects of epilepsy and neuroimaging profiles, higher high gamma augmentation at the resected language-dominant hemispheric area predicted a more severe postoperative decline in Core Language Score and Expressive Language Index. Conversely, the model incorporating picture naming-related high gamma augmentation predicted the change in Receptive Language Index with an r2 of 0.50. Higher high gamma augmentation independently predicted a more severe postoperative decline in Receptive Language Index. Ancillary regression analysis indicated that naming-related low gamma augmentation and alpha/beta attenuation likewise independently predicted a more severe Core Language Score decline. The machine learning-based prediction model suggested that naming-related high gamma augmentation, among all spectral responses used as predictors, most strongly contributed to the improved prediction of patients showing a >5-point Core Language Score decline (reflecting the lower 25th percentile among patients). We generated the model-based atlas visualizing sites, which, if resected, would lead to such a language decline. With a 5-fold cross-validation procedure, the auditory naming-based model predicted patients who had such a postoperative language decline with an accuracy of 0.80. The model indicated that virtual resection of an electrical stimulation mapping-defined language site would have increased the relative risk of the Core Language Score decline by 5.28 (95% confidence interval: 3.47-8.02). Especially, that of an electrical stimulation mapping-defined receptive language site would have maximized it to 15.90 (95% confidence interval: 9.59-26.33). In summary, naming-related spectral responses predict neuropsychological outcomes after epilepsy surgery. We have provided our prediction model as an open-source material, which will indicate the postoperative language function of future patients and facilitate external validation at tertiary epilepsy centres.
Keywords: event-related high gamma augmentation; high-frequency oscillations (HFOs); intracranial electroencephalography (iEEG) recording; paediatric epilepsy surgery; ripples.
© The Author(s) (2022). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Rosenow F, Lüders H.. Presurgical evaluation of epilepsy. Brain. 2001;124(Pt 9):1683–1700. - PubMed
-
- So EL, Alwaki A.. A guide for cortical electrical stimulation mapping. J Clin Neurophysiol. 2018;35(2):98–105. - PubMed
-
- Hamberger MJ, Seidel WT, Mckhann GM, Perrine K, Goodman RR.. Brain stimulation reveals critical auditory naming cortex. Brain. 2005;128(Pt 11):2742–2749. - PubMed
-
- Tate MC, Herbet G, Moritz-Gasser S, Tate JE, Duffau H.. Probabilistic map of critical functional regions of the human cerebral cortex: Broca’s area revisited. Brain. 2014;137(Pt 10):2773–2782. - PubMed
-
- Ojemann G, Ojemann J, Lettich E, Berger M.. Cortical language localization in left, dominant hemisphere: An electrical stimulation mapping investigation in 117 patients. J Neurosurg. 1989;71(3):316–326. - PubMed
