

Prognostic value of serum/plasma neurofilament light chain for COVID-19-associated mortality
- PMID: 35313387
- PMCID: PMC9082006
- DOI: 10.1002/acn3.51542
Prognostic value of serum/plasma neurofilament light chain for COVID-19-associated mortality
Abstract
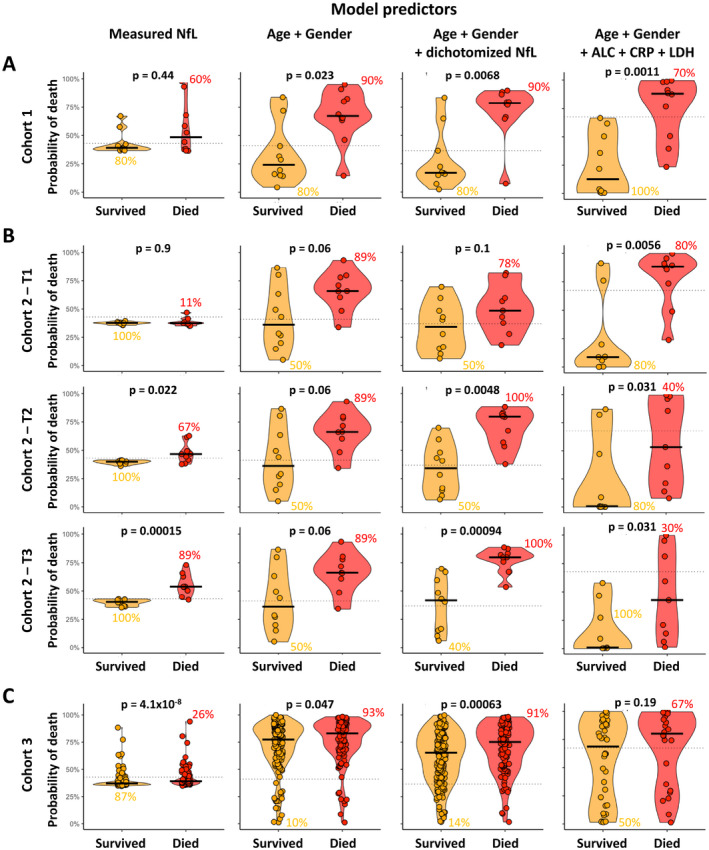
Objective: Given the continued spread of coronavirus 2, the early predictors of coronavirus disease 19 (COVID-19) associated mortality might improve patients' outcomes. Increased levels of circulating neurofilament light chain (NfL), a biomarker of neuronal injury, have been observed in severe COVID-19 patients. We investigated whether NfL provides non-redundant clinical value to previously identified predictors of COVID-19 mortality.
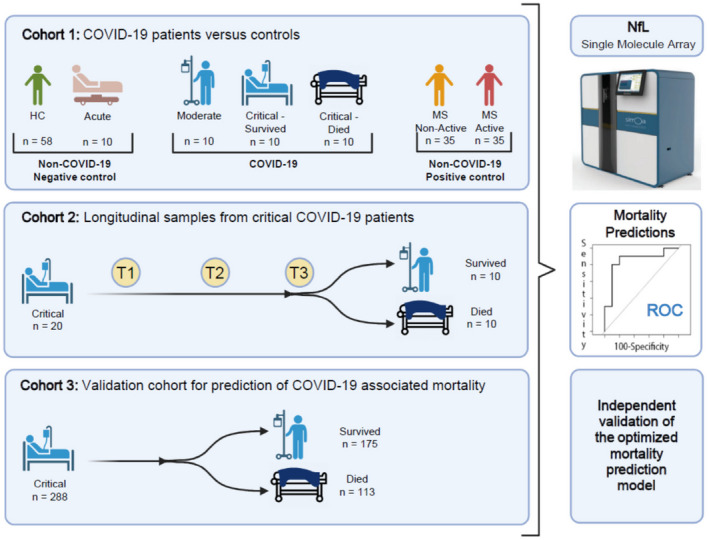
Methods: We measured serum or plasma NfL concentrations in a blinded fashion in 3 cohorts totaling 338 COVID-19 patients.
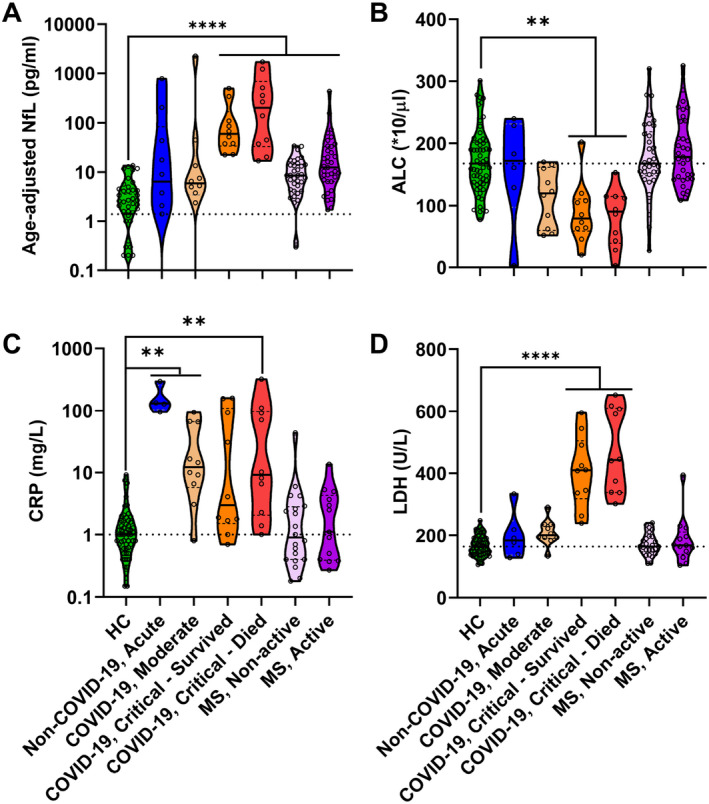
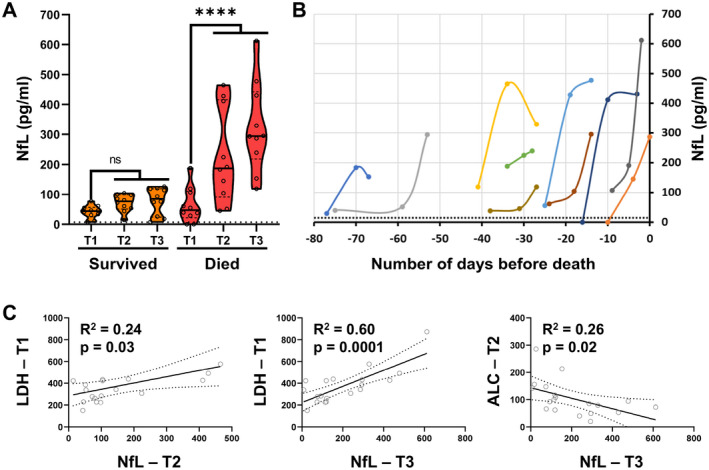
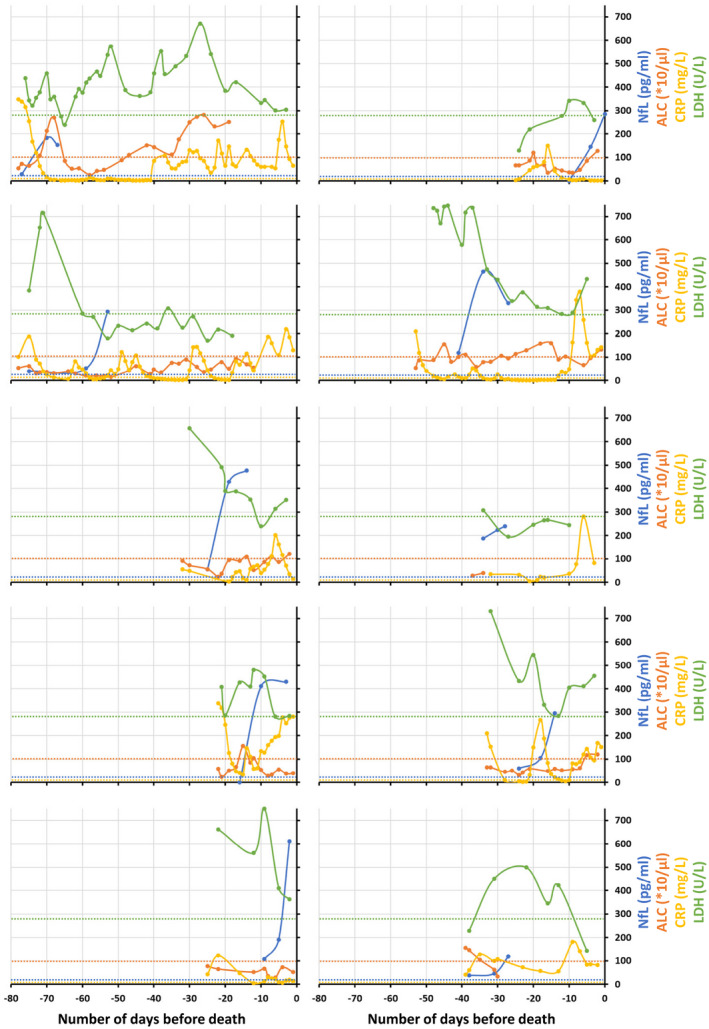
Results: In cohort 1, we found significantly elevated NfL levels only in critically ill COVID-19 patients. Longitudinal cohort 2 data showed that NfL is elevated late in the course of the disease, following the two other prognostic markers of COVID-19: decrease in absolute lymphocyte count (ALC) and increase in lactate dehydrogenase (LDH). Significant correlations between ALC and LDH abnormalities and subsequent rise of NfL implicate that the multi-organ failure is the most likely cause of neuronal injury in severe COVID-19 patients. The addition of NfL to age and gender in cohort 1 significantly improved the accuracy of mortality prediction and these improvements were validated in cohorts 2 and 3.
Interpretation: A substantial increase in serum/plasma NfL reproducibly enhanced COVID-19 mortality prediction. Combined with other prognostic markers, such as ALC and LDH that are routinely measured in ICU patients, NfL measurements might be useful to identify the patients at a high risk of COVID-19-associated mortality, who might still benefit from escalated care.
© 2022 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Update of
-
Prognostic Value of Serum/Plasma Neurofilament Light Chain for COVID-19 Associated Mortality.medRxiv [Preprint]. 2022 Jan 14:2022.01.13.22269244. doi: 10.1101/2022.01.13.22269244. medRxiv. 2022. Update in: Ann Clin Transl Neurol. 2022 May;9(5):622-632. doi: 10.1002/acn3.51542. PMID: 35075461 Free PMC article. Updated. Preprint.
References
-
- COVID Live – Coronavirus Statistics – Worldometer. https://www.worldometers.info/coronavirus/
-
- Gaetani L, Blennow K, Calabresi P, di Filippo M, Parnetti L, Zetterberg H. Neurofilament light chain as a biomarker in neurological disorders. J Neurol Neurosurg Psychiatry. 2019;90(8):870‐881. - PubMed
-
- Kan CW, Rivnak AJ, Campbell TG, et al. Isolation and detection of single molecules on paramagnetic beads using sequential fluid flows in microfabricated polymer array assemblies. Lab Chip. 2012;12(5):977‐985. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical