

This is a preprint.
A conserved immune trajectory of recovery in hospitalized COVID-19 patients
- PMID: 35313585
- PMCID: PMC8936097
- DOI: 10.1101/2022.03.15.484467
A conserved immune trajectory of recovery in hospitalized COVID-19 patients
Update in
-
Mass cytometry reveals a conserved immune trajectory of recovery in hospitalized COVID-19 patients.Immunity. 2022 Jul 12;55(7):1284-1298.e3. doi: 10.1016/j.immuni.2022.06.004. Epub 2022 Jun 7. Immunity. 2022. PMID: 35779527 Free PMC article.
Abstract
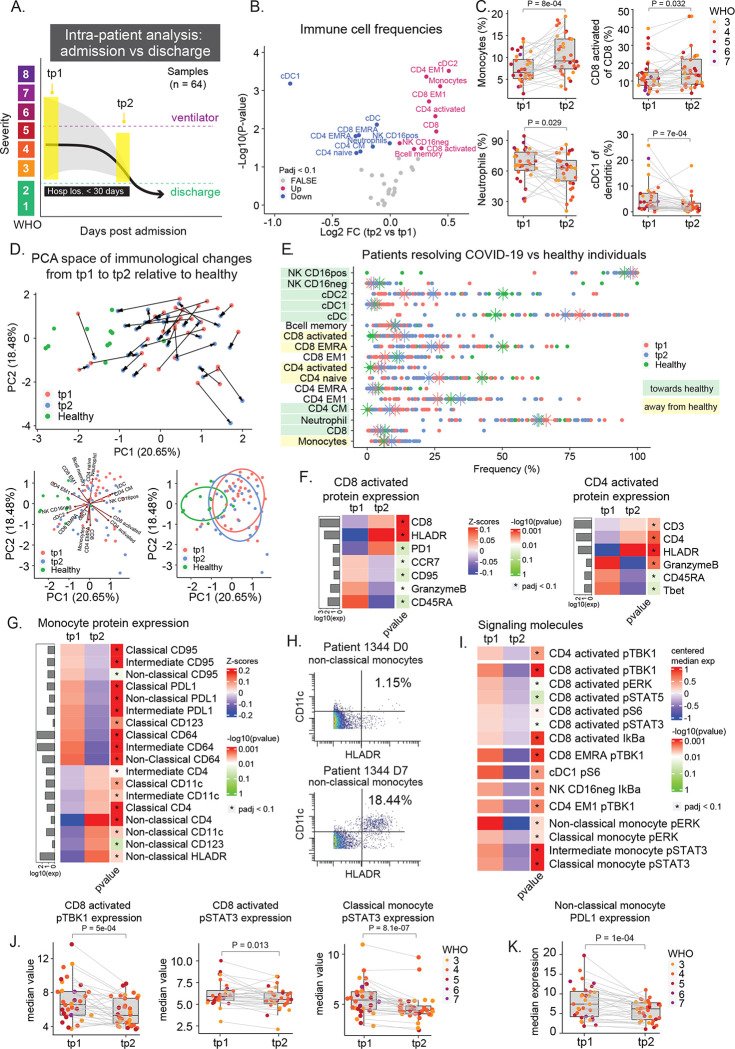
Many studies have provided insights into the immune response to COVID-19; however, little is known about the immunological changes and immune signaling occurring during COVID-19 resolution. Individual heterogeneity and variable disease resolution timelines obscure unifying immune characteristics. Here, we collected and profiled >200 longitudinal peripheral blood samples from patients hospitalized with COVID-19, with other respiratory infections, and healthy individuals, using mass cytometry to measure immune cells and signaling states at single cell resolution. COVID-19 patients showed a unique immune composition and an early, coordinated and elevated immune cell signaling profile, which correlated with early hospital discharge. Intra-patient time course analysis tied to clinically relevant events of recovery revealed a conserved set of immunological processes that accompany, and are unique to, disease resolution and discharge. This immunological process, together with additional changes in CD4 regulatory T cells and basophils, accompanies recovery from respiratory failure and is associated with better clinical outcomes at the time of admission. Our work elucidates the biological timeline of immune recovery from COVID-19 and provides insights into the fundamental processes of COVID-19 resolution in hospitalized patients.
Figures





References
-
- Allen Breanna M., Hiam Kamir J., Burnett Cassandra E., Venida Anthony, DeBarge Rachel, Tenvooren Iliana, Marquez Diana M., Cho Nam Woo, Carmi Yaron, and Spitzer Matthew H.. 2020. “Systemic Dysfunction and Plasticity of the Immune Macroenvironment in Cancer Models.” Nature Medicine 26 (7): 1125–34. - PMC - PubMed
-
- Asano Takaki, Boisson Bertrand, Onodi Fanny, Matuozzo Daniela, Moncada-Velez Marcela, Maglorius Renkilaraj Majistor Raj Luxman, Zhang Peng, et al. 2021. “X-Linked Recessive TLR7 Deficiency in ~1% of Men under 60 Years Old with Life-Threatening COVID-19.” Science Immunology 6 (62). 10.1126/sciimmunol.abl4348. - DOI - PMC - PubMed
-
- Centers for Disease Control and Prevention. 2021. “CDC COVID Data Tracker.” Trends in Number of COVID-19 Cases and Deaths in the US Reported to CDC, by State/Territory. November 9, 2021. https://covid.cdc.gov/covid-data-tracker/#trends_dailydeaths.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials