

Intraoperative application of yellow fluorescence in resection of intramedullary spinal canal ependymoma
- PMID: 35313772
- PMCID: PMC8943562
- DOI: 10.1177/03000605221082889
Intraoperative application of yellow fluorescence in resection of intramedullary spinal canal ependymoma
Abstract
Background: Spinal ependymoma is the most common intramedullary tumor in adults. This study was performed to evaluate whether intraoperative yellow fluorescence use enhances our ability to identify the tumor margin and residual tumor tissue in intramedullary spinal cord ependymoma resection. We also evaluated patients' clinical conditions at a 3-month follow-up.
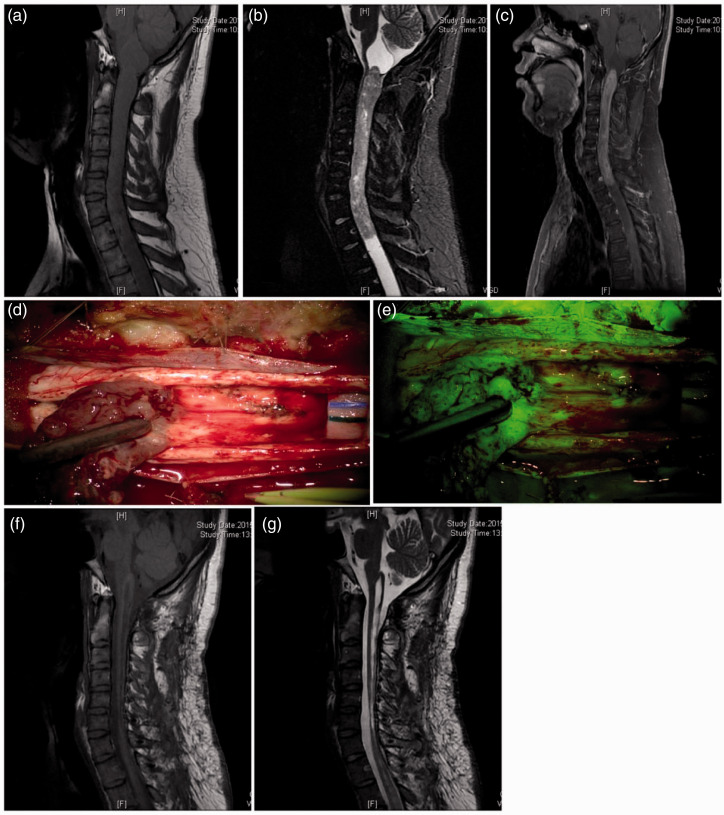
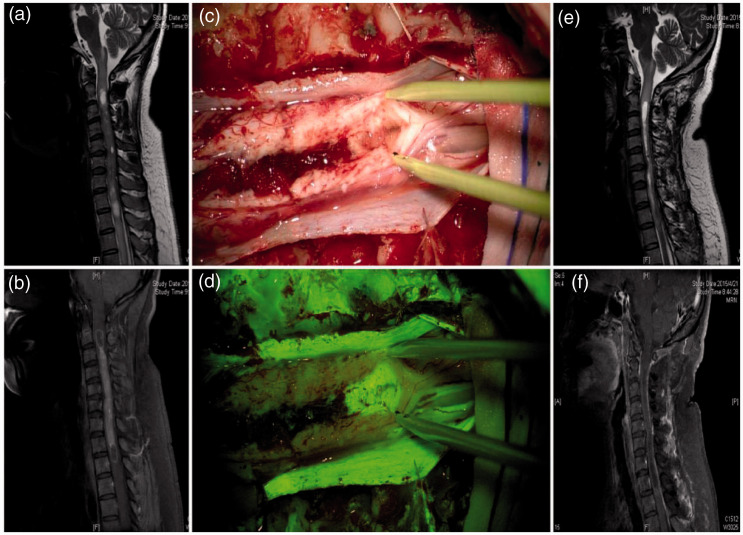
Methods: We retrospectively evaluated 56 patients with intramedullary ependymoma. Thirty minutes before anesthesia, the patients received intravenous sodium fluorescein injections. Tumor resection was performed under two illumination modes, traditional white light and yellow fluorescence, and the residual tumor tissue was detected. Magnetic resonance imaging was performed 3 months postoperatively to observe the tumor resection outcome and residual tumor tissue. The McCormick spinal cord function grade was evaluated preoperatively and 3 months postoperatively.
Results: The total resection rate was 100.0% in all patients. Nine patients had no significant fluorescence imaging. After 3 months, patients with a spinal function grade of I to IV showed significant spinal function improvement. Magnetic resonance imaging showed no residual tumor tissue or recurrence.
Conclusion: Sodium fluorescein aids in total excision of intramedullary spinal cord ependymoma and intraoperative residual tumor tissue identification. At the 3-month follow-up, the patients' functional outcome in the fluorescein group was good.
Keywords: Spinal cord tumor; ependymoma; functional outcome; neurosurgery; residual tumor; yellow fluorescence.
Figures

Similar articles
-
Quantitative Analysis of Near-Infrared Indocyanine Green Videoangiography for Predicting Functional Outcomes After Spinal Intramedullary Ependymoma Resection.Oper Neurosurg. 2019 Nov 1;17(5):531-539. doi: 10.1093/ons/opz040. Oper Neurosurg. 2019. PMID: 30888018
-
Factors associated with progression-free survival and long-term neurological outcome after resection of intramedullary spinal cord tumors: analysis of 101 consecutive cases.J Neurosurg Spine. 2009 Nov;11(5):591-9. doi: 10.3171/2009.4.SPINE08159. J Neurosurg Spine. 2009. PMID: 19929363
-
Laser fluorescence spectroscopy in surgical treatment of intramedullary tumors: experience of the Burdenko Neurosurgery Center.Zh Vopr Neirokhir Im N N Burdenko. 2023;87(5):21-27. doi: 10.17116/neiro20238705121. Zh Vopr Neirokhir Im N N Burdenko. 2023. PMID: 37830465 English, Russian.
-
Intradural Extramedullary Nonconus Nonfilum Spinal Ependymomas: Report of a Rare Variant and Newer Insights into Their Histogenesis with Proposal of a Classification Scheme and a Management Algorithm Based on a Review of Literature.World Neurosurg. 2020 Feb;134:323-336. doi: 10.1016/j.wneu.2019.10.152. Epub 2019 Nov 1. World Neurosurg. 2020. PMID: 31682991 Review.
-
Giant intradural myxopapillary ependymoma: review of literature.BMJ Case Rep. 2021 Jan 28;14(1):e239453. doi: 10.1136/bcr-2020-239453. BMJ Case Rep. 2021. PMID: 33509888 Free PMC article. Review.
Cited by
-
Fluorescence-guided resection of intradural spinal tumors: a systematic review and meta-analysis.Neurosurg Rev. 2023 Dec 12;47(1):10. doi: 10.1007/s10143-023-02230-x. Neurosurg Rev. 2023. PMID: 38085385
References
-
- Ehrhardt A, Stepp H, Irion K, et al.. Fluorescence detection of human malignancies using incoherent light systems. Med La App 2003; 18: 27–35.
-
- Ewelt C, Nemes A, Senner V, et al.. Fluorescence in neurosurgery: its diagnostic and therapeutic use. Review of the literature. J Photochem Photobiol B-Biol 2015; 148: 302–309. - PubMed
-
- Keil VC, Schmitt AJ, Martin S, et al.. Optimising treatment strategies in spinal ependymoma based on 20 years of experience at a single centre. J Clin Neurosci 2016; 29: 52–58. - PubMed
-
- Kim D, Kim J, Choi SH, et al.. Differentiation between Intramedullary spinal ependymoma and astrocytoma: comparative MRI analysis. Clin Radiol 2014; 69: 29–35. - PubMed
-
- Kukreja S, Ambekar S, Sharma M, et al.. Outcome predictors in the management of spinal myxopapillary ependymoma: an integrative survival analysis. World Neurosurg 2015; 83: 852–859. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
