

The effects of preoperative rehabilitation on pain and functional outcome after total knee arthroplasty: a meta-analysis of randomized controlled trials
- PMID: 35313897
- PMCID: PMC8935773
- DOI: 10.1186/s13018-022-03066-9
The effects of preoperative rehabilitation on pain and functional outcome after total knee arthroplasty: a meta-analysis of randomized controlled trials
Abstract
Background: There have been controversial findings for the effectiveness of rehabilitation before operation after total knee arthroplasty (TKA). This study aimed to conduct an updated, comprehensive systematic review. On that basis, the review was to be combined with meta-analysis to measure the effects of rehabilitation before operation on functions and pain after TKA.
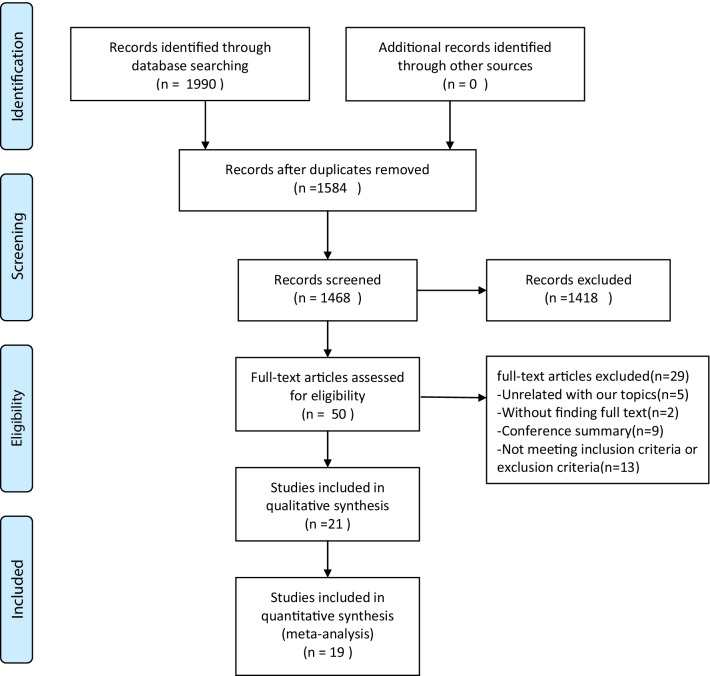
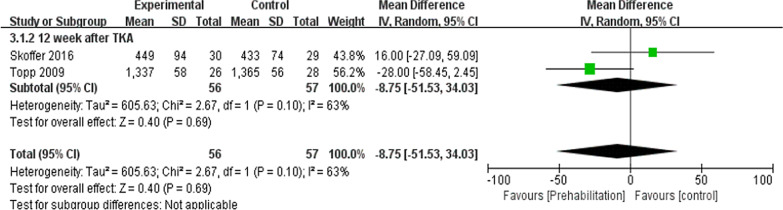
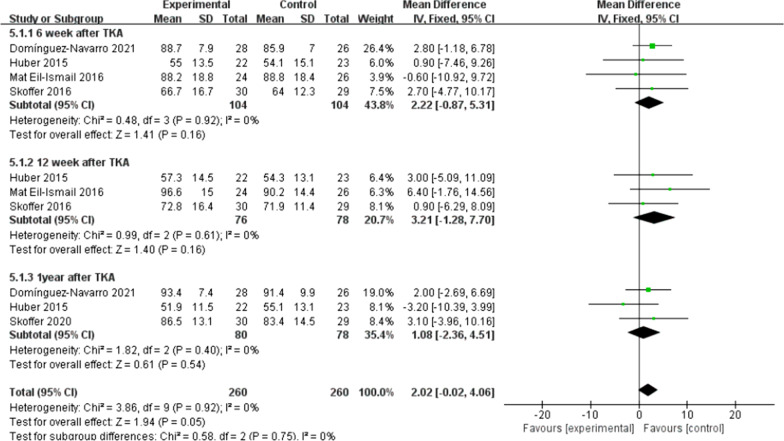
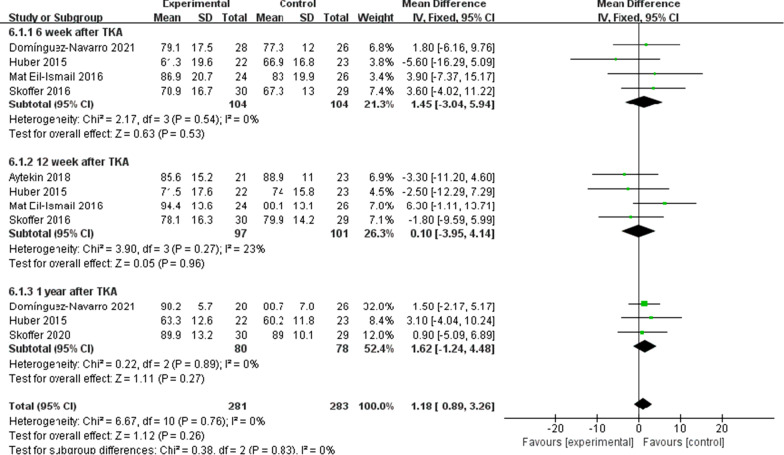
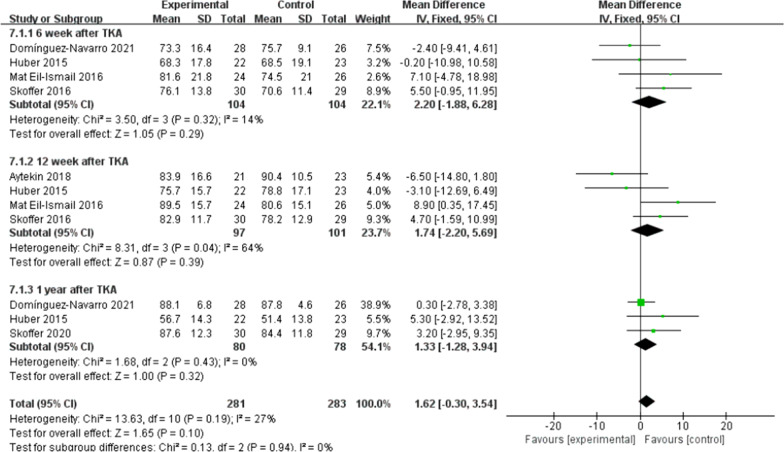
Methods: Articles were searched by using Central Register of Controlled Trials (CENTRAL), Web of Science, EMBASE, Cochrane, Pubmed, CNKI, Wanfang, Weipu and the Chinese Biomedical Database from the beginning to December 10, 2021. The major outcomes included pain, knee flexion and extension, as well as knee range of motion (ROM). Secondary outcomes included timed-up-and-go (TUG), 6-min walk, and patient-reported functional outcome (the Knee Injury and Osteoarthritis Outcome Score (KOOS) or Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)). Third outcomes included the length of hospital stay.
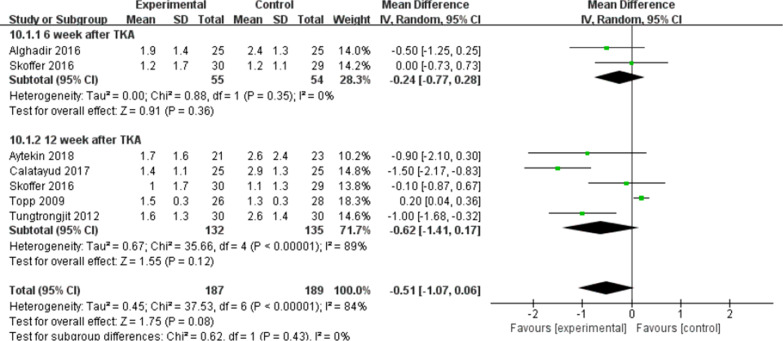
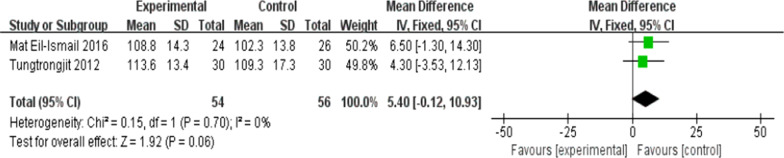
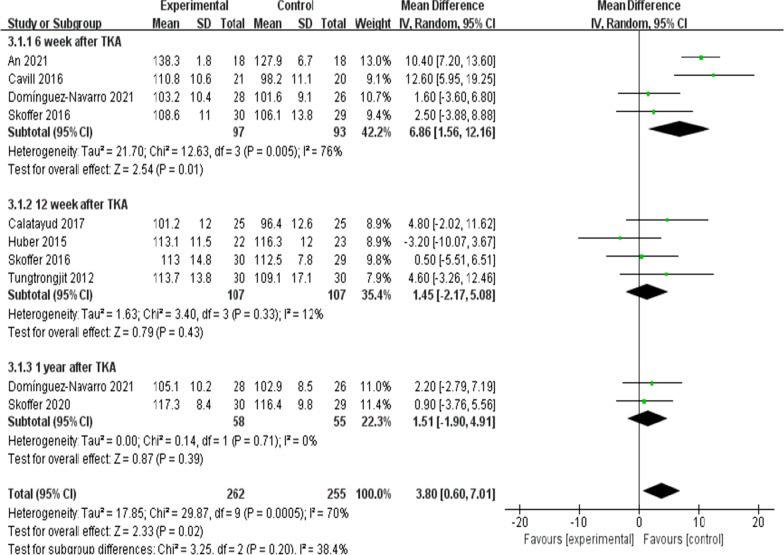
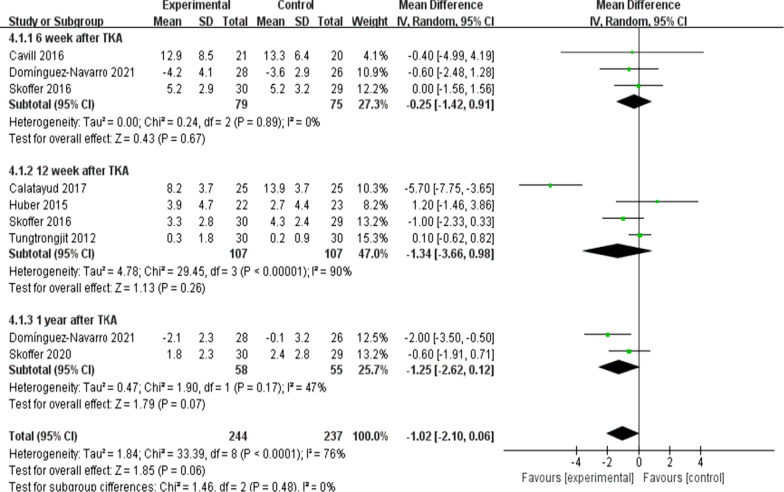
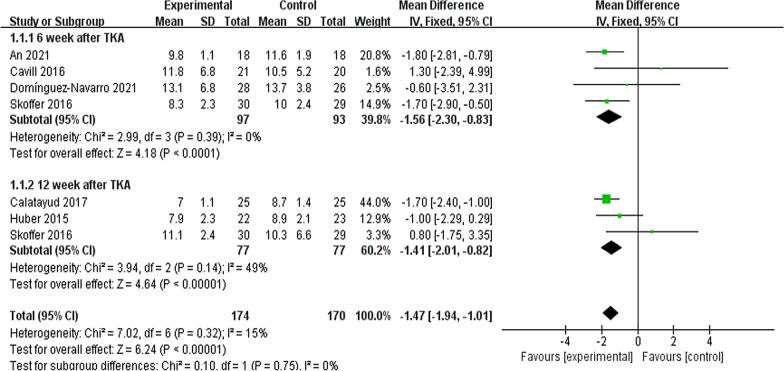
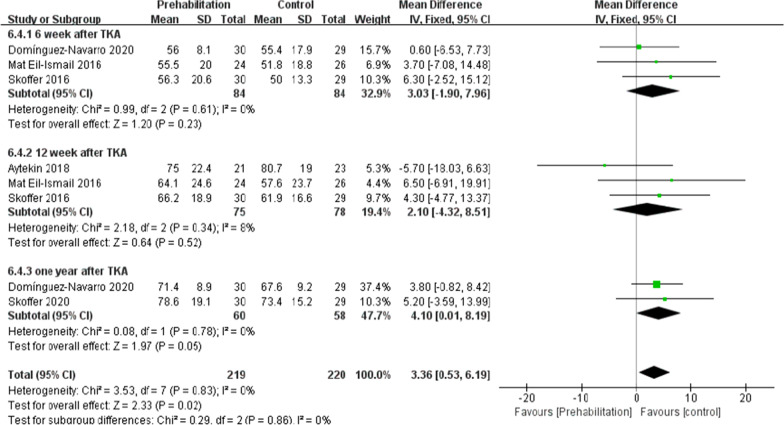
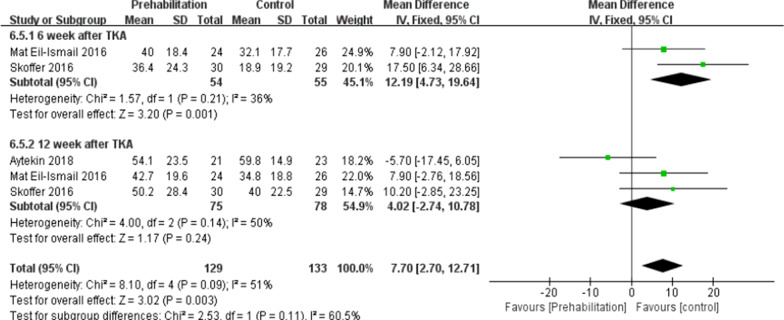
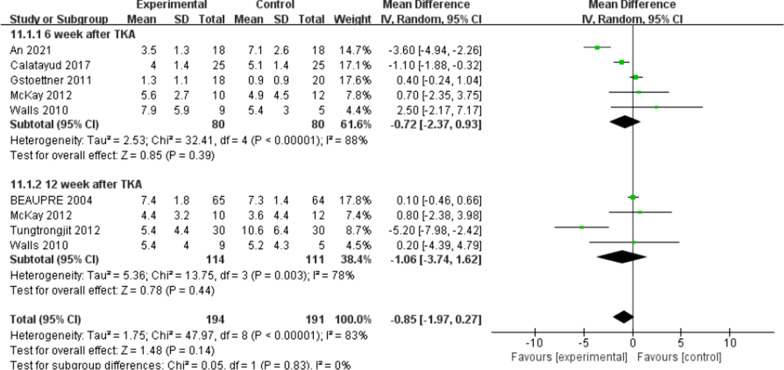
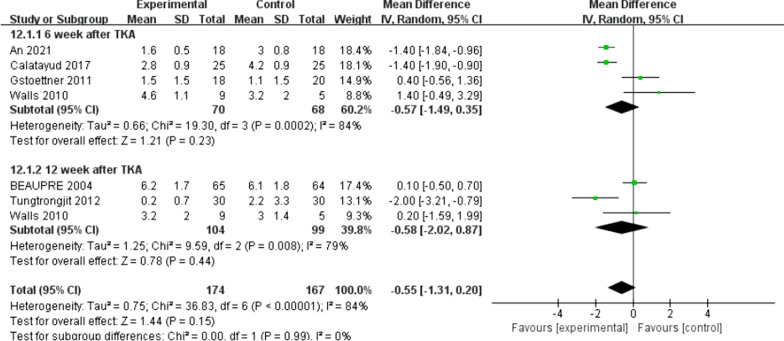
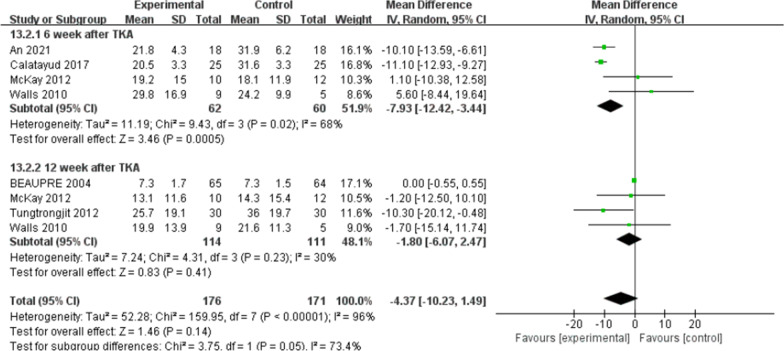
Results: Nineteen studies recruiting 1008 patients satisfied with the inclusion criteria. Significant difference was identified in knee flexion, TUG, KOOS (knee-associated life quality and functions in sports and recreation), as well as the length of hospital stay (P < 0.05). Insignificant statistical difference was identified in pain, 6-min walk, ROM, knee extension, KOOS (pain, symptoms and function of daily living) after TKA between the two groups. No difference was found between the groups in WOMAC.
Conclusions: Preoperative rehabilitation could significantly shorten hospital stay, whereas there is not any conclusive evidence of the improvement of postoperative functions. Accordingly, in-depth high-quality studies should be conducted to confirm the effectiveness of preoperative rehabilitation in patients having received TKA.
Keywords: Meta-analysis; Randomized controlled trials; Rehabilitation; Total knee arthroplasty.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Comparison of Kinematic Alignment and Mechanical Alignment in Total Knee Arthroplasty: A Meta-analysis of Randomized Controlled Clinical Trials.Orthop Surg. 2020 Dec;12(6):1567-1578. doi: 10.1111/os.12826. Epub 2020 Oct 25. Orthop Surg. 2020. PMID: 33099892 Free PMC article. Review.
-
A systematic review and meta-analysis of the effect of preoperative exercise intervention on rehabilitation after total knee arthroplasty.Ann Palliat Med. 2021 Oct;10(10):10986-10996. doi: 10.21037/apm-21-2670. Ann Palliat Med. 2021. PMID: 34763461
-
Effects of lower-limb active resistance exercise on mobility, physical function, knee strength and pain intensity in patients with total knee arthroplasty: a systematic review and meta-analysis.BMC Musculoskelet Disord. 2024 Sep 12;25(1):730. doi: 10.1186/s12891-024-07845-9. BMC Musculoskelet Disord. 2024. PMID: 39267026 Free PMC article.
-
Functional outcomes and length of stay with early and high-intensity rehabilitation after simultaneous bilateral total knee arthroplasty.J Back Musculoskelet Rehabil. 2023;36(1):107-115. doi: 10.3233/BMR-210238. J Back Musculoskelet Rehabil. 2023. PMID: 35848009
-
The Effectiveness of Virtual Reality, Augmented Reality, and Mixed Reality Rehabilitation in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis.J Arthroplasty. 2024 Mar;39(3):582-590.e4. doi: 10.1016/j.arth.2023.08.051. Epub 2023 Aug 19. J Arthroplasty. 2024. PMID: 37598785
Cited by
-
Effect of total knee arthroplasty on quadriceps and hamstring muscle recovery in individuals with knee osteoarthritis: A proposed systematic review and meta-analysis protocol.MethodsX. 2024 Nov 15;13:103057. doi: 10.1016/j.mex.2024.103057. eCollection 2024 Dec. MethodsX. 2024. PMID: 39650115 Free PMC article.
-
Pathogen Distribution, Drug Resistance, and Postoperative High-Quality Nursing Intervention Effectiveness in Knee Osteoarthritis Patients After Knee Arthroplasty With Postoperative Infection.J Multidiscip Healthc. 2025 Feb 17;18:891-902. doi: 10.2147/JMDH.S506445. eCollection 2025. J Multidiscip Healthc. 2025. PMID: 39990634 Free PMC article.
-
Cryotherapy for Rehabilitation After Total Knee Arthroplasty: A Comprehensive Systematic Review and Meta-Analysis.Orthop Surg. 2024 Dec;16(12):2897-2915. doi: 10.1111/os.14266. Epub 2024 Oct 14. Orthop Surg. 2024. PMID: 39402654 Free PMC article.
-
Risk factors associated with the failure of day surgery for total knee arthroplasty a multivariate logistic regression analysis.Front Surg. 2025 Jun 26;12:1597068. doi: 10.3389/fsurg.2025.1597068. eCollection 2025. Front Surg. 2025. PMID: 40642453 Free PMC article.
-
Comparison of the efficacy of robot-assisted total knee arthroplasty in patients with knee osteoarthritis with varying severity deformity.J Orthop Surg Res. 2024 Dec 24;19(1):872. doi: 10.1186/s13018-024-05372-w. J Orthop Surg Res. 2024. PMID: 39719605 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
