

Alternative autologous and biologic conduits have worse outcomes than prosthetic grafts for infrainguinal bypass in patients with chronic limb-threatening ischemia
- PMID: 35314304
- PMCID: PMC10804316
- DOI: 10.1016/j.jvs.2022.03.006
Alternative autologous and biologic conduits have worse outcomes than prosthetic grafts for infrainguinal bypass in patients with chronic limb-threatening ischemia
Abstract
Objective: Single segment great saphenous vein (GSV) is the preferred conduit in infrainguinal bypass. Alternative autologous conduits (AAC) and nonautologous biologic conduits (NABC) are thought to be a better alternative to traditional prosthetic conduits (PC) in the absence of GSV. In this study we analyzed the outcomes of these alternative conduits in lower extremity bypasses (LEB) in patients with chronic limb-threatening ischemia.
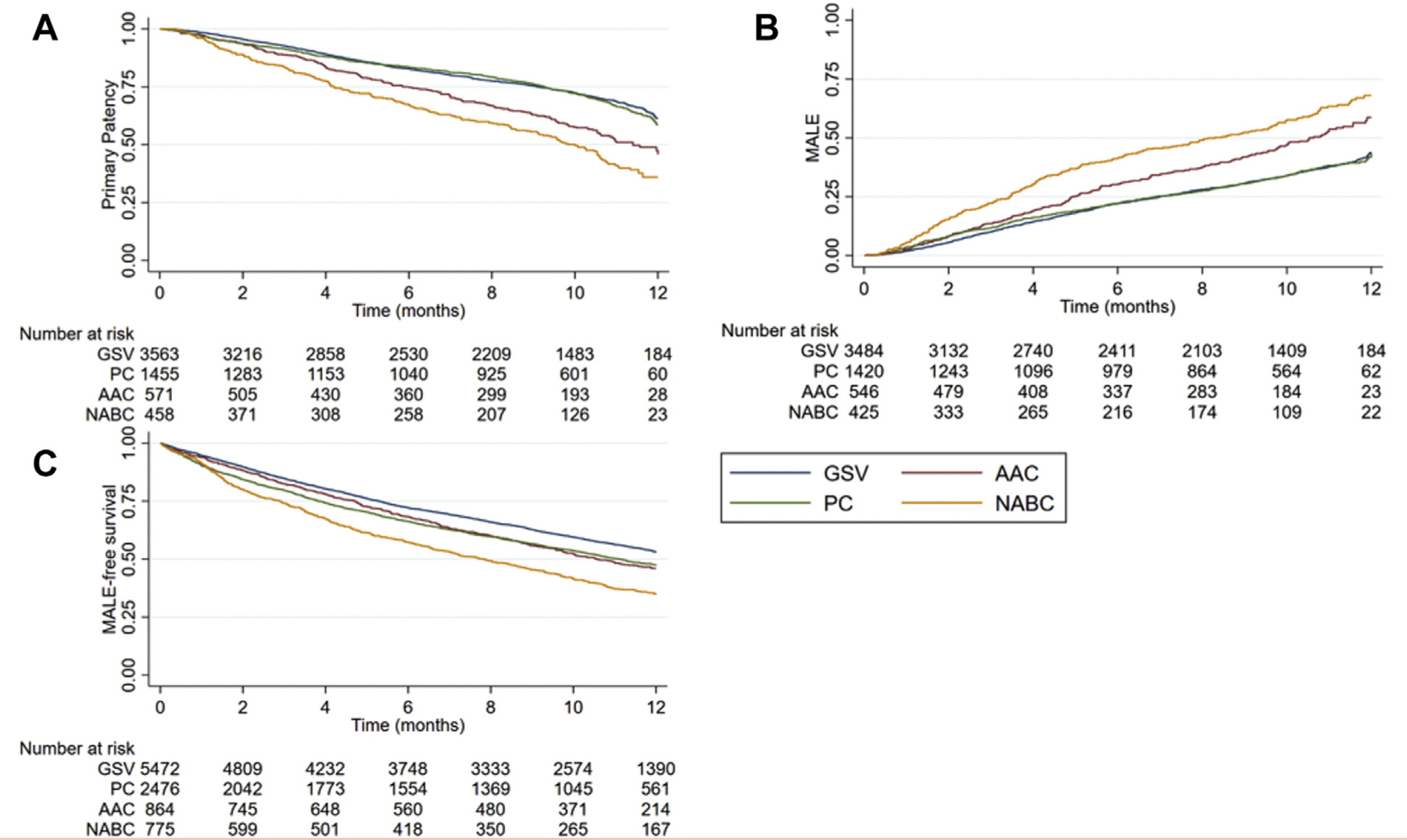
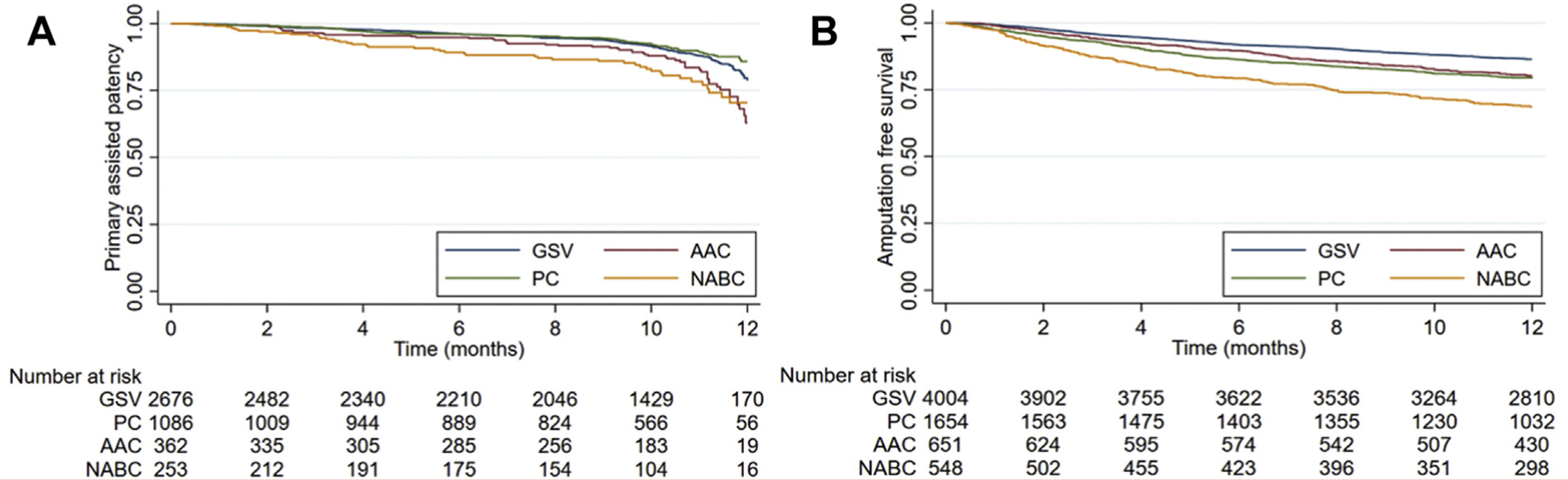
Methods: The Vascular Quality Initiative LEB database from 2003 to 2020 was queried for this study, to identify LEB in patients with chronic limb-threatening ischemia. Primary outcomes were graft patency, major adverse limb events (MALE), and MALE-free survival at 1 year. Standard statistical methods were used as appropriate.
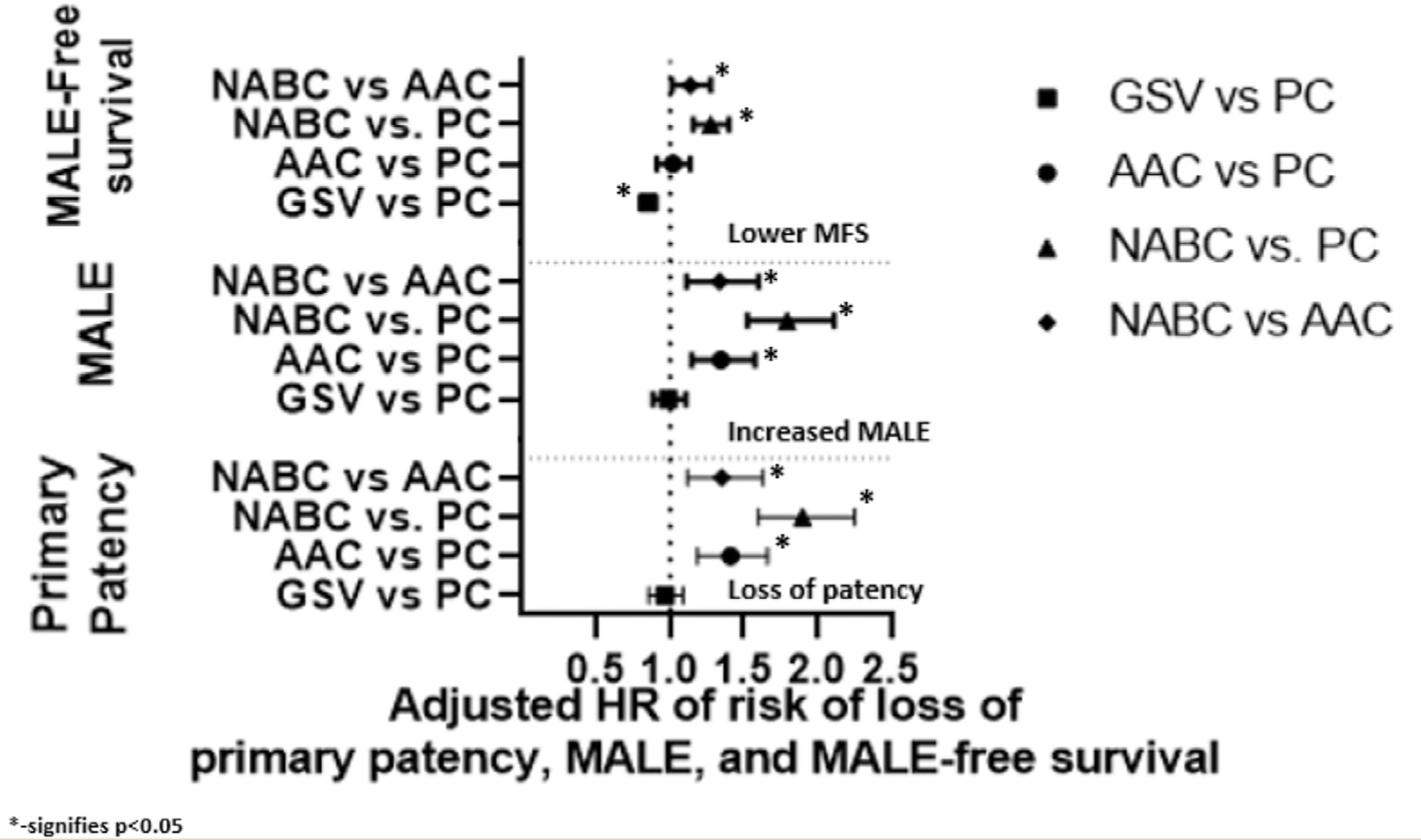
Results: We identified 22,671 LEB procedures (12,810 GSV, 6002 PC, 1907 AAC, and 1952 NABC). Compared with the GSV group, the other conduit patients were significantly older, had more comorbidities, had an increased rate of prior lower extremity interventions, had a higher rate of infrageniculate bypass targets, and were less ambulatory at baseline. The PC, AAC, and NABC groups had significantly higher rates of postoperative morbidity compared with the GSV group. The PC group had a higher 30-day mortality compared with the GSV, AAC, and NABC groups (3% PC vs 2% GSV, 2% AAC, 2% NABC; P = .049). Both PC and NABC had higher 1-year mortality compared with GSV and AAC (13% PC and 13% NABC vs 10% GSV, 10% AAC; P = .02). In an adjusted Cox regression model (stratified by infrageniculate target and adjusted for age, comorbidities, and prior vascular interventions) PC was not significantly different from GSV, but AAC (hazard ratio [HR], 1.41; 95% confidence interval [CI], 1.19-1.67; P < .001) and NABC (HR, 1.9; 95% CI, 1.61-2.25; P < .001) were associated with an increased risk of loss of primary patency. A similar association with MALE was observed: both AAC (HR, 1.35; 95% CI, 1.15-1.58; P < .001) and NABC (HR, 1.8; 95% CI, 1.53-2.11; P < .001) were associated with an increased risk of MALE compared with GSV; PC was not significantly different from GSV.
Conclusions: In the absence of GSV, alternative conduits (autologous or nonautologous biologic) do not confer a benefit with regard to graft patency or MALE compared with PCs. Increased operating time or costs associated with the use of these conduits is not justified based on this study.
Keywords: Alternative conduit; Loss of patency; Lower extremity bypass; Major adverse limb events; Outcomes.
Copyright © 2022 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
References
-
- Pereira CE, Albers M, Romiti M, Brochado-Neto FC, Pereira CAB. Meta-analysis of femoropopliteal bypass grafts for lower extremity arterial insufficiency. J Vasc Surg 2006;44:510–7. - PubMed
-
- Taylor LM, Edwards JM, Porter JM. Present status of reversed vein bypass grafting: five-year results of a modern series. J Vasc Surg 1990;11:193–205. - PubMed
-
- Veith FJ, Gupta SK, Ascer E, White-Flores S, Samson RH, Scher LA, et al. Six-year prospective multicenter randomized comparison of autologous saphenous vein and expanded polytetrafluoroethylene grafts in infrainguinal arterial reconstructions. J Vasc Surg 1986;3: 104–14. - PubMed
-
- Faries PL, LoGerfo FW, Arora S, Hook S, Pulling MC, Akbari CM, et al. A comparative study of alternative conduits for lower extremity revascularization: all-autogenous conduit versus prosthetic grafts. J Vasc Surg 2000;32:1080–90. - PubMed
-
- Avgerinos ED, Sachdev U, Naddaf A, Doucet DR, Mohapatra A, Leers SA, et al. Autologous alternative veins may not provide better outcomes than prosthetic conduits for below-knee bypass when great saphenous vein is unavailable. J Vasc Surg 2015;62:385–91. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
