

Evaluation of a health and social care programme to improve outcomes following critical illness: a multicentre study
- PMID: 35314485
- PMCID: PMC9872253
- DOI: 10.1136/thoraxjnl-2021-218428
Evaluation of a health and social care programme to improve outcomes following critical illness: a multicentre study
Abstract
Rationale: At present, clinicians aiming to support patients through the challenges after critical care have limited evidence to base interventions.
Objectives: Evaluate a multicentre integrated health and social care intervention for critical care survivors. A process evaluation assessed factors influencing the programme implementation.
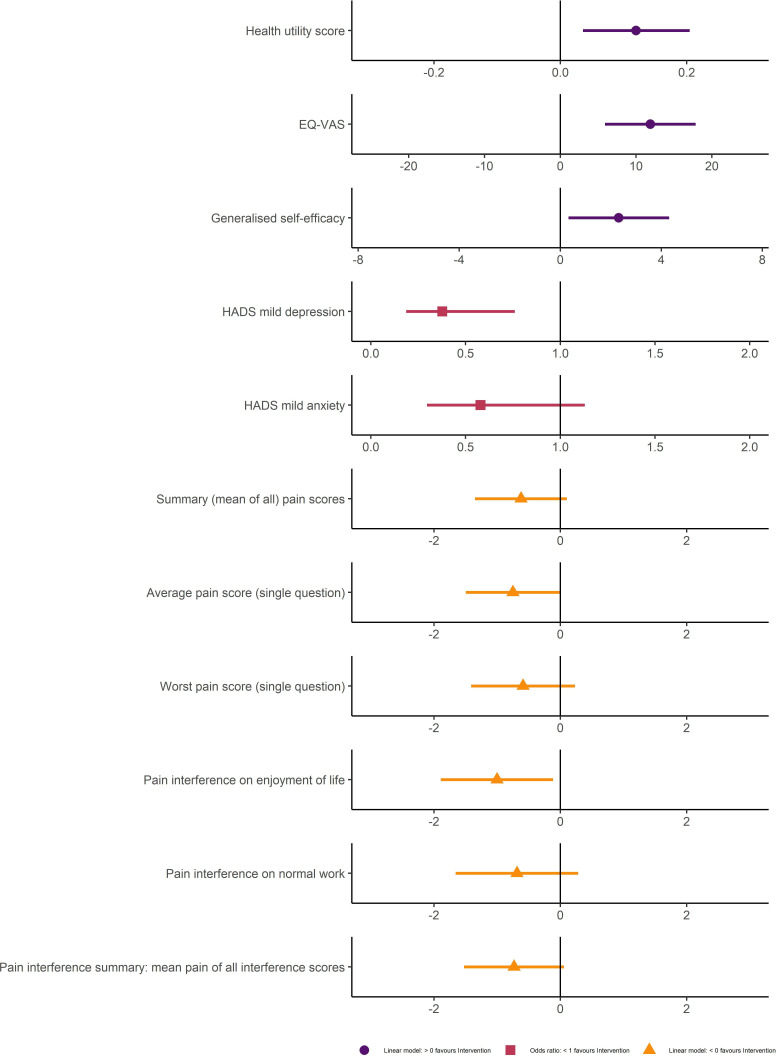
Methods: This study evaluated the impact of the Intensive Care Syndrome: Promoting Independence and Return to Employment (InS:PIRE) programme. We compared patients who attended this programme with a usual care cohort from the same time period across nine hospital sites in Scotland. The primary outcome was health-related quality of life (HRQoL) measured via the EuroQol 5-dimension 5-level instrument, at 12 months post hospital discharge. Secondary outcome measures included self-efficacy, depression, anxiety and pain.
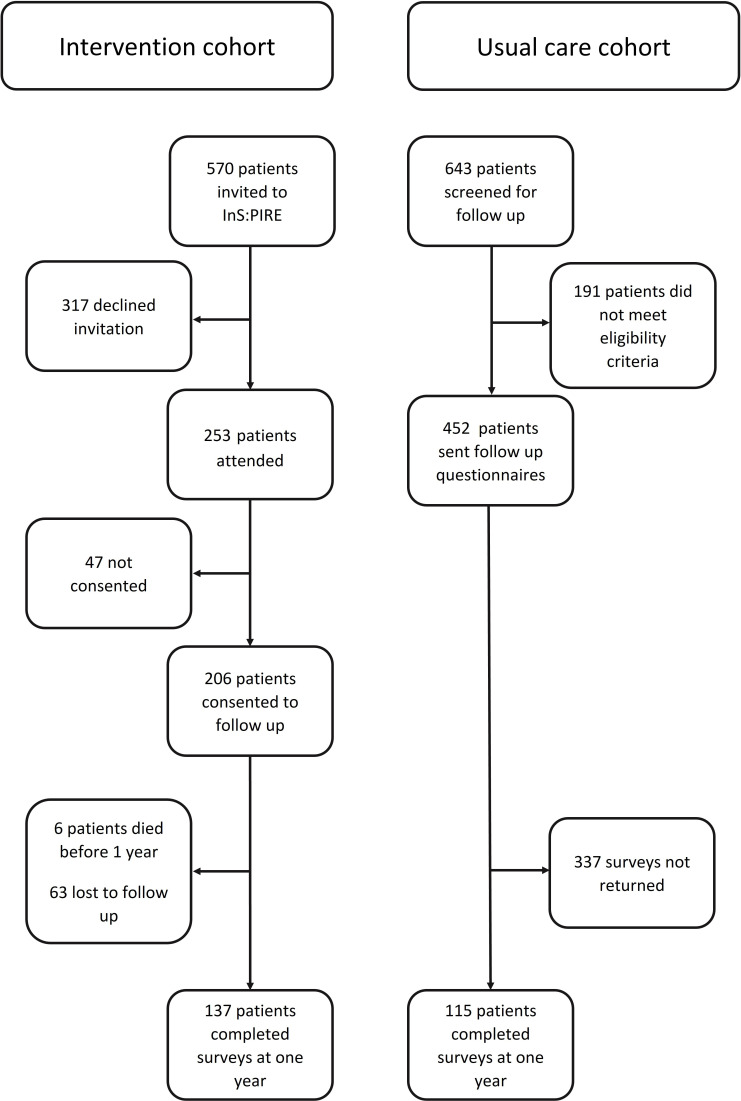
Results: 137 patients who received the InS:PIRE intervention completed outcome measures at 12 months. In the usual care cohort, 115 patients completed the measures. The two cohorts had similar baseline demographics. After adjustment, there was a significant absolute increase in HRQoL in the intervention cohort in relation to the usual care cohort (0.12, 95% CI 0.04 to 0.20, p=0.01). Patients in the InS:PIRE cohort also reported self-efficacy scores that were 7.7% higher (2.32 points higher, 95% CI 0.32 to 4.31, p=0.02), fewer symptoms of depression (OR 0.38, 95% CI 0.19 to 0.76, p=0.01) and similar symptoms of anxiety (OR 0.58, 95% CI 0.30 to 1.13, p=0.11). There was no significant difference in overall pain experience. Key facilitators for implementation were: integration with inpatient care, organisational engagement, flexibility to service inclusion; key barriers were: funding, staff availability and venue availability.
Conclusions: This multicentre evaluation of a health and social care programme designed for survivors of critical illness appears to show benefit at 12 months following hospital discharge.
Keywords: ARDS; critical care; pulmonary rehabilitation.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
A multicentre evaluation exploring the impact of an integrated health and social care intervention for the caregivers of ICU survivors.Crit Care. 2022 May 24;26(1):152. doi: 10.1186/s13054-022-04014-z. Crit Care. 2022. PMID: 35610616 Free PMC article.
-
Intensive Care Syndrome: Promoting Independence and Return to Employment (InS:PIRE). Early evaluation of a complex intervention.PLoS One. 2017 Nov 29;12(11):e0188028. doi: 10.1371/journal.pone.0188028. eCollection 2017. PLoS One. 2017. PMID: 29186177 Free PMC article.
-
Effectiveness of a programme of exercise on physical function in survivors of critical illness following discharge from the ICU: study protocol for a randomised controlled trial (REVIVE).Trials. 2014 Apr 27;15:146. doi: 10.1186/1745-6215-15-146. Trials. 2014. PMID: 24767671 Free PMC article. Clinical Trial.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: a systematic review and meta-analysis.BMJ Open. 2018 May 5;8(5):e019998. doi: 10.1136/bmjopen-2017-019998. BMJ Open. 2018. PMID: 29730622 Free PMC article.
Cited by
-
Medication-related problems in critical care survivors: a systematic review.Eur J Hosp Pharm. 2023 Sep;30(5):250-256. doi: 10.1136/ejhpharm-2023-003715. Epub 2023 May 4. Eur J Hosp Pharm. 2023. PMID: 37142386 Free PMC article.
-
Could an integrated model of health and social care after critical illness reduce socioeconomic disparities in outcomes? A Bayesian analysis.BJA Open. 2024 Jan 31;9:100259. doi: 10.1016/j.bjao.2024.100259. eCollection 2024 Mar. BJA Open. 2024. PMID: 38322488 Free PMC article.
-
Interviews with primary care physicians identify unmet transition needs after ICU.Crit Care. 2022 Aug 15;26(1):248. doi: 10.1186/s13054-022-04125-7. Crit Care. 2022. PMID: 35971153 Free PMC article.
-
Association Between Caregiver Strain and Emergency Health Care Resource Utilization in Survivors of Critical Illness.Chest. 2025 Mar;167(3):768-771. doi: 10.1016/j.chest.2024.08.057. Epub 2024 Oct 3. Chest. 2025. PMID: 39368736 Free PMC article. No abstract available.
-
Factors Associated With New Analgesic Requirements Following Critical Illness.J Intensive Care Med. 2024 Jun;39(6):550-557. doi: 10.1177/08850666231219916. Epub 2023 Dec 12. J Intensive Care Med. 2024. PMID: 38087427 Free PMC article.
References
-
- Pandharipande PP, Girard TD, Jackson JC. Delirium is an independent predictor of long-term cognitive impairment: results from the brain ICU (bringing to light the risk factors and incidence of neuropsychological dysfunction in ICU survivors) study. D16 randomized and observational studies in critical care. American thoracic Society, 2013: A5237–A.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources