

Diabetes Mellitus Is a Possible Risk Factor for Nodo-paranodopathy With Antiparanodal Autoantibodies
- PMID: 35314491
- PMCID: PMC8936686
- DOI: 10.1212/NXI.0000000000001163
Diabetes Mellitus Is a Possible Risk Factor for Nodo-paranodopathy With Antiparanodal Autoantibodies
Abstract
Background and objectives: Nodo-paranodopathies are peripheral neuropathies with dysfunction of the node of Ranvier. Affected patients who are seropositive for antibodies against adhesion molecules like contactin-1 and neurofascin show distinct clinical features and a disruption of the paranodal complex. An axoglial dysjunction is also a characteristic finding of diabetic neuropathy. Here, we aim to investigate a possible association of antibody-mediated nodo-paranodopathy and diabetes mellitus (DM).
Methods: We retrospectively analyzed clinical data of 227 patients with chronic inflammatory demyelinating polyradiculoneuropathy and Guillain-Barré syndrome from multiple centers in Germany who had undergone diagnostic testing for antiparanodal antibodies targeting neurofascin-155, pan-neurofascin, contactin-1-associated protein 1, and contactin-1. To study possible direct pathogenic effects of antiparanodal antibodies, we performed immunofluorescence binding assays on human pancreatic tissue sections.
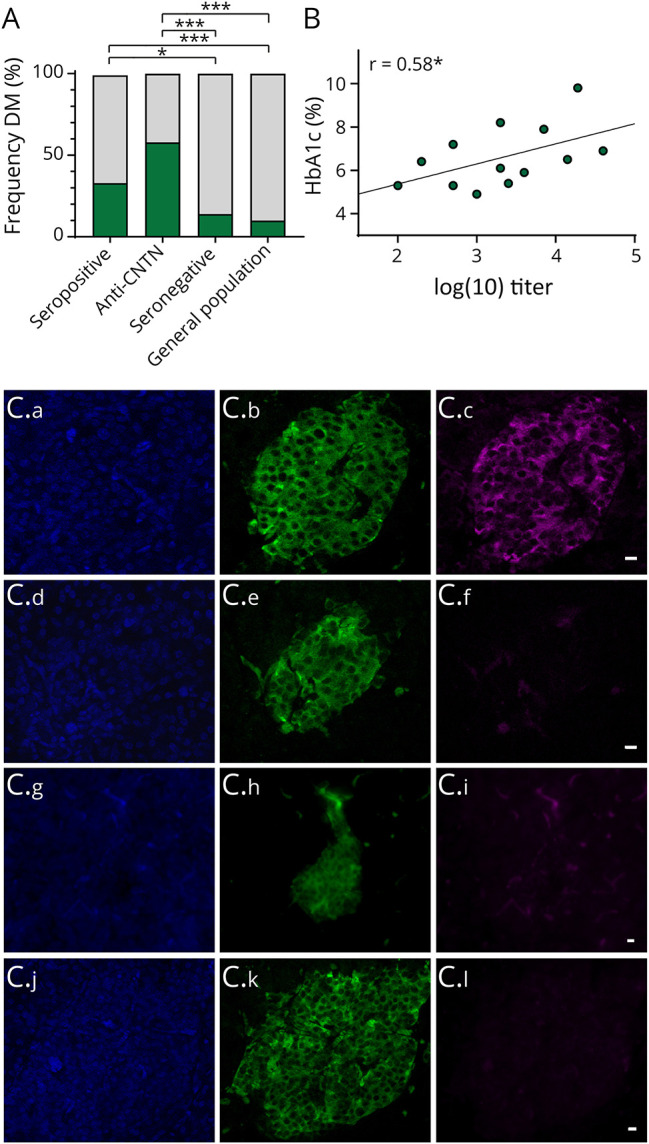
Results: The frequency of DM was 33.3% in seropositive patients and thus higher compared with seronegative patients (14.1%, OR = 3.04, 95% CI = 1.31-6.80). The relative risk of DM in seropositive patients was 3.4-fold higher compared with the general German population. Seropositive patients with DM most frequently harbored anti-contactin-1 antibodies and had higher antibody titers than seropositive patients without DM. The diagnosis of DM preceded the onset of neuropathy in seropositive patients. No immunoreactivity of antiparanodal antibodies against pancreatic tissue was detected.
Discussion: We report an association of nodo-paranodopathy and DM. Our results suggest that DM may be a potential risk factor for predisposing to developing nodo-paranodopathy and argue against DM being induced by the autoantibodies. Our findings set the basis for further research investigating underlying immunopathogenetic connections.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Pascual-Goni E, Martin-Aguilar L, Querol L. Autoantibodies in chronic inflammatory demyelinating polyradiculoneuropathy. Curr Opin Neurol. 2019;32(5):651-657. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials