

Development and Validation of the Pediatric Hypersomnolence Survey
- PMID: 35314496
- PMCID: PMC9141629
- DOI: 10.1212/WNL.0000000000200187
Development and Validation of the Pediatric Hypersomnolence Survey
Abstract
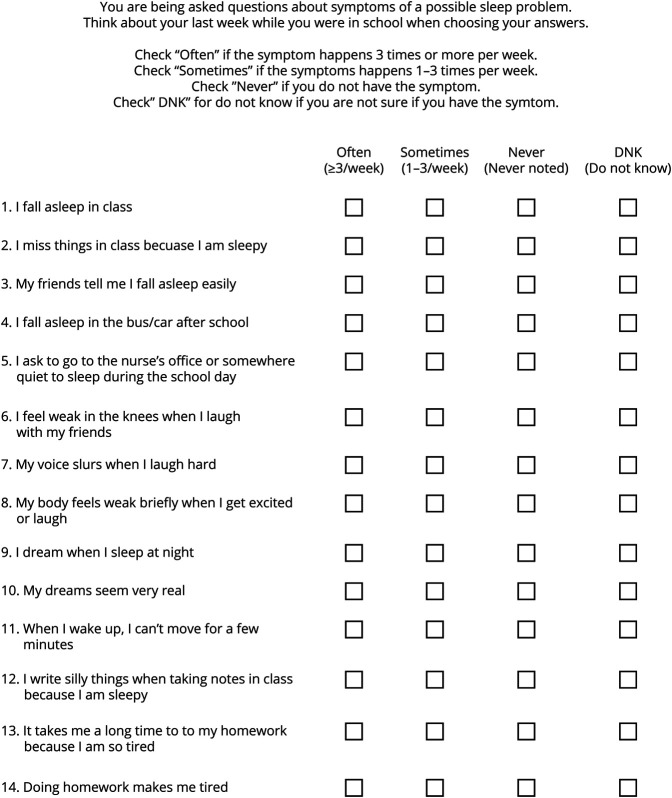
Background and objectives: Narcolepsy and idiopathic hypersomnia usually begin in early adolescence, but diagnostic delays ranging from 5 to 10 years are common, affecting disease burden. To improve early identification of these treatable conditions, we developed and validated the Pediatric Hypersomnolence Survey (PHS).
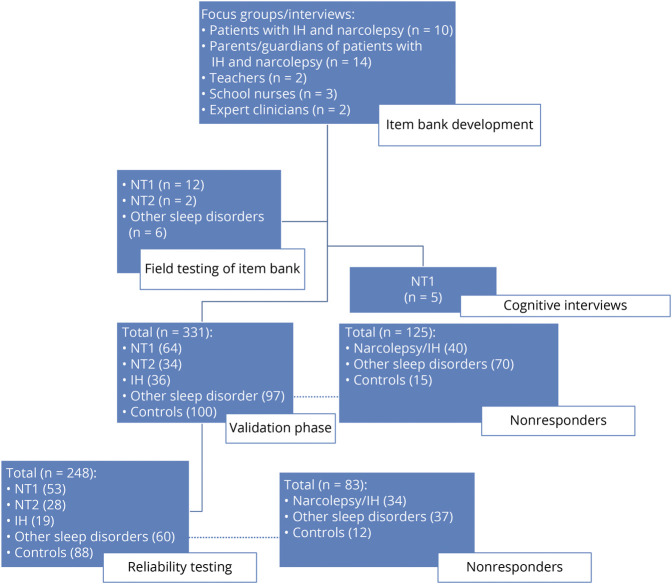
Methods: Content was developed through literature review, patient focus groups, interviews with experts in the field, and field testing. We then validated the 14-item self-reported survey across 3 hospitals and web recruitment from patient groups. In the validation phase, we recruited a total of 331 participants (patients with narcolepsy type 1 [n = 64], narcolepsy type 2 [n = 34], idiopathic hypersomnia [n = 36], and other sleep disorders [n = 97] and healthy controls [n = 100], ages 8-18 years) to complete the survey. We assessed a range of psychometric properties, including discriminant diagnostic validity for CNS disorders of hypersomnolence using receiver operating characteristic curve analysis and reliability across a 1-week period.
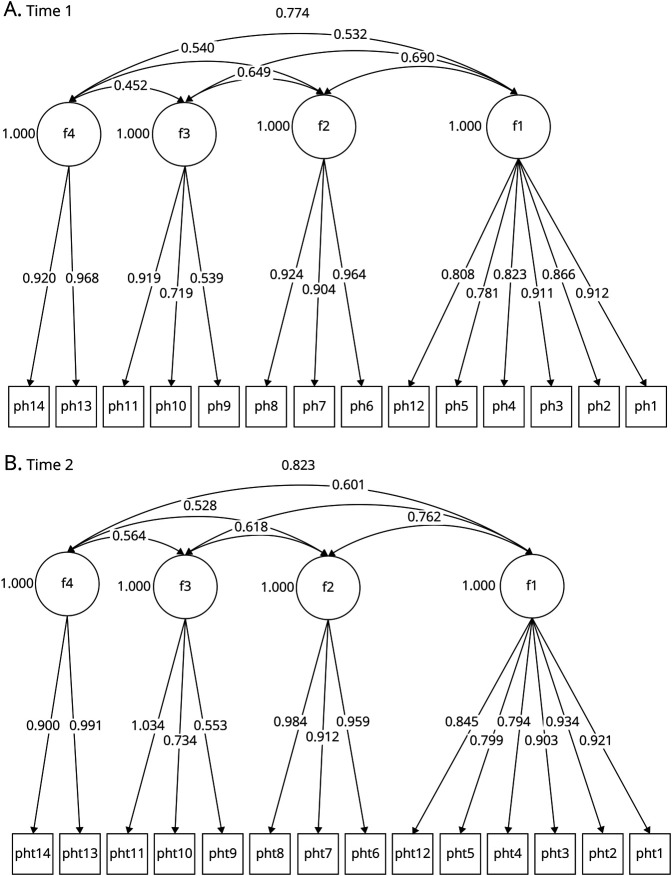
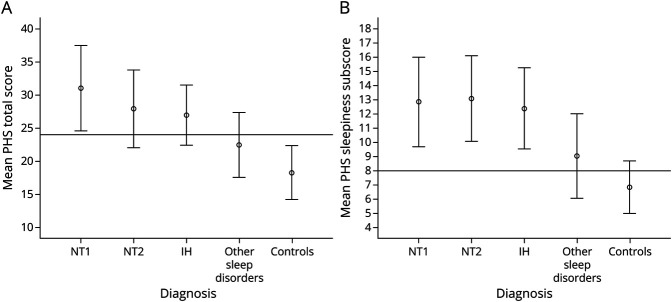
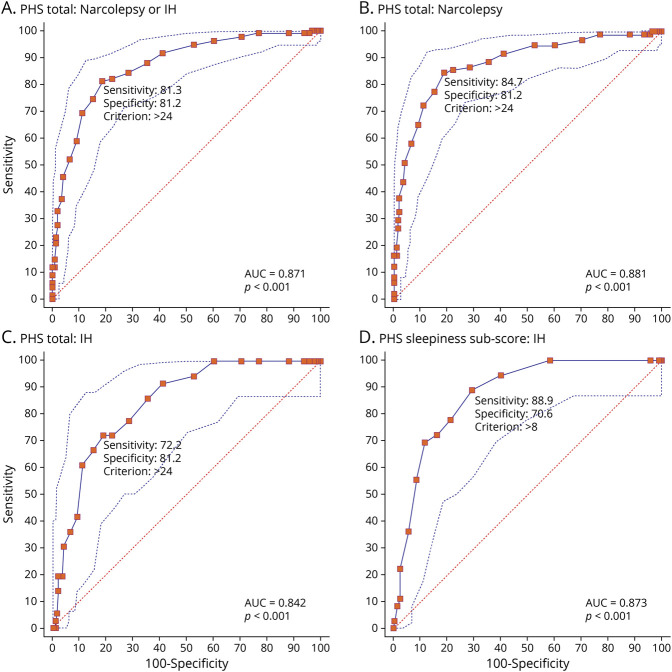
Results: Confirmatory factor analysis indicated a 4-domain solution with good reliability expressed by satisfactory omega values. Across groups, the PHS total score showed appropriate positive correlations with other validated surveys of sleepiness (r = 0.65-0.78, p < 0.001) and negative correlations with multiple sleep latency test measures (mean sleep latency: r = -0.27, p = 0.006; number of sleep-onset REM periods: r = 0.26, p = 0.007). Compared to controls and patients with other sleep disorders, the area under the curve for participants with narcolepsy or idiopathic hypersomnia was 0.87 (standard error 0.02, 95% CI 0.83-0.91) with high sensitivity (81.3, 95% CI 73.7%-87.5%) and specificity (81.2%, 95 CI 75.1%-86.4%). Test-retest reliability was r = 0.87.
Discussion: The PHS is a valid and reliable tool for clinicians to identify pediatric patients with narcolepsy and idiopathic hypersomnia. Implemented in clinical practice, the PHS will potentially decrease diagnostic delays and time to treatment, ultimately reducing disease burden for these debilitating conditions.
Classification of evidence: This study provides Class III evidence that the PHS accurately identifies patients with central disorders of hypersomnolence.
© 2022 American Academy of Neurology.
Figures
References
-
- Thorpy MJ, Krieger AC. Delayed diagnosis of narcolepsy: characterization and impact. Sleep Med. 2014;15(5):502-507. - PubMed
-
- Luca G, Haba-Rubio J, Dauvilliers Y, et al. . Clinical, polysomnographic and genome-wide association analyses of narcolepsy with cataplexy: a European Narcolepsy Network study. J Sleep Res. 2013;22(5):482-495. - PubMed
-
- American Academy of Sleep Medicine. International Classification of Sleep Disorders–Third Edition (ICSD-3). American Academy of Sleep Medicine; 2014.
-
- Rosenberg R, Kim AY. The AWAKEN survey: knowledge of narcolepsy among physicians and the general population. Postgrad Med. 2014;126(1):78-86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials