

Forthcoming Step in Gastric Cancer Prevention: How Can Risk Stratification Be Combined with Endoscopic Screening for Gastric Cancer?
- PMID: 35314519
- PMCID: PMC9668507
- DOI: 10.5009/gnl210313
Forthcoming Step in Gastric Cancer Prevention: How Can Risk Stratification Be Combined with Endoscopic Screening for Gastric Cancer?
Abstract
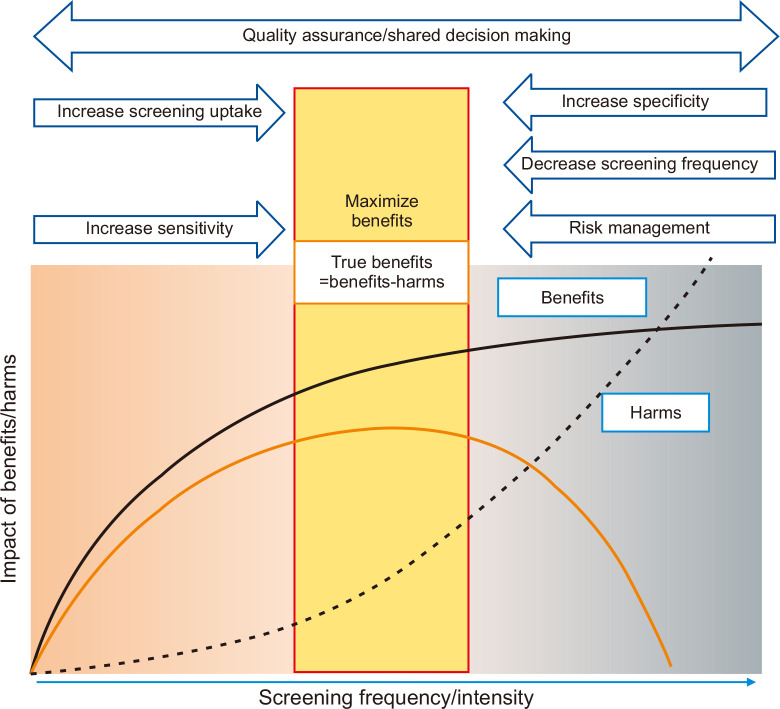
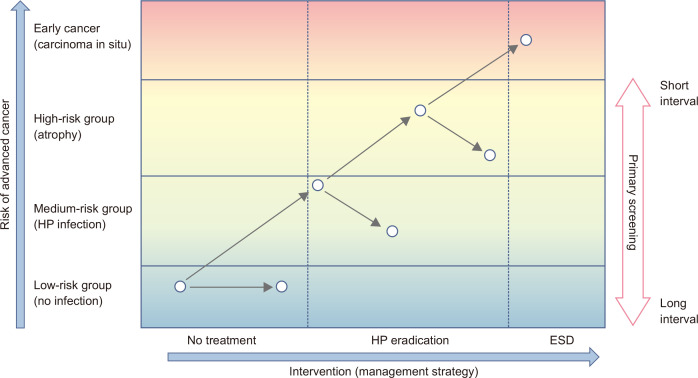
Although the concern for gastric cancer prevention has increased, gastric cancer has remained a heavy burden worldwide and is not just a local issue in East Asian countries. However, as several screening programs (listed below) have shown some success, it is important to determine whether the situation is changing in some other countries and whether similar methods should be recommended. Endoscopic screening has been performed as a national program in South Korea and Japan, and the results have shown a reduction in gastric cancer mortality. Although the efficacy of Helicobacter pylori eradication has been established, the efficacy of the screen-and-treat strategy is presently being evaluated in randomized controlled trials. The serum pepsinogen test and endoscopic examination can divide high-risk subjects with severe gastric atrophy from average-risk subjects. Risk stratification is anticipated to contribute to an efficient method of prediction of gastric cancer development when combined with endoscopic screening. Countries with a high incidence rate should realize the immediate need to reduce gastric cancer death directly by endoscopic screening and should recognize screen-and-treat as a second option to reduce future risk. However, all forms of gastric cancer prevention programs have some harms and potential to increase unnecessary examinations. A balance of the benefits and harms should be always considered. Although further study is needed to obtain sufficient evidence for gastric cancer prevention, the best available method should be examined in the context of each country.
Keywords:
Endoscopes;
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Screening of gastric cancer in Asia.Best Pract Res Clin Gastroenterol. 2015 Dec;29(6):895-905. doi: 10.1016/j.bpg.2015.09.013. Epub 2015 Sep 25. Best Pract Res Clin Gastroenterol. 2015. PMID: 26651251 Review.
-
Population based Helicobacter pylori screening and eradication: advances versus side effects.Curr Pharm Des. 2014;20(28):4501-9. doi: 10.2174/13816128113196660733. Curr Pharm Des. 2014. PMID: 24180403 Review.
-
Update version of the Japanese Guidelines for Gastric Cancer Screening.Jpn J Clin Oncol. 2018 Jul 1;48(7):673-683. doi: 10.1093/jjco/hyy077. Jpn J Clin Oncol. 2018. PMID: 29889263
-
Screening and eradication of Helicobacter pylori for gastric cancer prevention: the Taipei global consensus.Gut. 2020 Dec;69(12):2093-2112. doi: 10.1136/gutjnl-2020-322368. Epub 2020 Oct 1. Gut. 2020. PMID: 33004546
-
Asia-Pacific consensus guidelines on gastric cancer prevention.J Gastroenterol Hepatol. 2008 Mar;23(3):351-65. doi: 10.1111/j.1440-1746.2008.05314.x. J Gastroenterol Hepatol. 2008. PMID: 18318820
Cited by
-
Cancer screening programs in South-east Asia and Western Pacific.BMC Health Serv Res. 2024 Jan 18;24(1):102. doi: 10.1186/s12913-023-10327-8. BMC Health Serv Res. 2024. PMID: 38238704 Free PMC article. Review.
-
Cost-effectiveness of adding a Helicobacter pylori antibody test to the upper gastrointestinal series in gastric cancer screening at the workplace.Environ Occup Health Pract. 2023 Dec 8;5(1):2023-0010-OA. doi: 10.1539/eohp.2023-0010-OA. eCollection 2023. Environ Occup Health Pract. 2023. PMID: 40059928 Free PMC article.
-
Clinical value of serum pepsinogen in the diagnosis and treatment of gastric diseases.World J Gastrointest Oncol. 2023 Jul 15;15(7):1174-1181. doi: 10.4251/wjgo.v15.i7.1174. World J Gastrointest Oncol. 2023. PMID: 37546552 Free PMC article. Review.
-
A DSC Test for the Early Detection of Neoplastic Gastric Lesions in a Medium-Risk Gastric Cancer Area.Int J Mol Sci. 2023 Feb 7;24(4):3290. doi: 10.3390/ijms24043290. Int J Mol Sci. 2023. PMID: 36834698 Free PMC article.
References
-
- International Agency for Research on Cancer (IARC), author Cancer Today, 2020 [Internet] IARC; Lyon: c2020. [cited 2020 Oct 3]. Available from: https://gco.iarc.fr/today/home .
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
