

Successful pregnancy and delivery after a vitrified-warmed embryo transfer in a woman with Kallmann syndrome: A case report and literature review
- PMID: 35314524
- PMCID: PMC9071358
- DOI: 10.5387/fms.2021-09
Successful pregnancy and delivery after a vitrified-warmed embryo transfer in a woman with Kallmann syndrome: A case report and literature review
Abstract
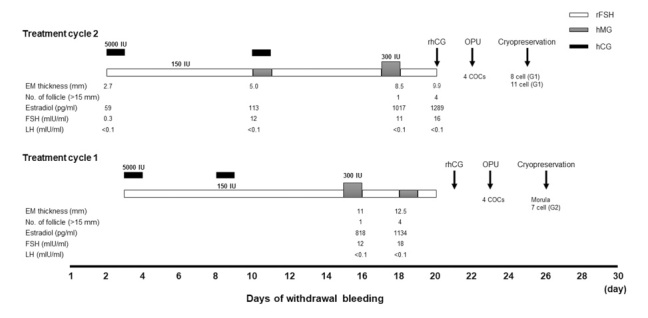
Kallmann syndrome, a congenital disorder of idiopathic hypogonadotropic hypogonadism associated with anosmia, results in infertility because of anovulation. Assisted reproductive technology (ART) is considered when optimal ovulation induction therapy is difficult or when several cycles of ovulation induction therapy do not result in pregnancy. However, evidence is lacking regarding the optimal ART treatment for Kallmann syndrome. We report the case of a 33-year-old woman who successfully achieved pregnancy and delivery after ART treatment. At 29 years old, she was diagnosed with Kallmann syndrome due to hypothalamic amenorrhea and anosmia. At 33 years old, she revisited the hospital, desiring a child after one year of infertility. Due to anovulation, she was treated with gonadotropin therapy, but controlling follicular development was difficult, and thus ART treatment was initiated. The controlled ovarian stimulation (COS) protocol for ART treatment employed gonadotropins, recombinant follicular stimulating hormone/human menopausal gonadotropin plus human chorionic gonadotropin, to promote follicular growth. Four oocytes were retrieved, and two cleaved embryos were vitrified and cryopreserved. After vitrified-warmed embryo transfer of a morula stage embryo in a hormone replacement cycle, pregnancy was achieved but resulted in a miscarriage. A second oocyte retrieval was performed under the same COS; four oocytes were retrieved, and two cleaved embryos were vitrified and cryopreserved. Further, a pregnancy was achieved through the vitrified warmed embryo transfer. At 40 weeks and 6 days of gestation, a baby boy weighing 3,344 g with an Apgar score of 7/8 was delivered vaginally. The mother's postpartum course and neonate were free from adverse events. For women with Kallmann syndrome, ART treatment and selective embryo cryopreservation may be a reasonable and safe option.
Keywords: Kallmann syndrome; assisted reproductive technology; frozen-thawed embryo transfer; gonadotropin therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Successful pregnancy by vitrified-warmed embryo transfer for a woman with Kallmann syndrome.Reprod Med Biol. 2015 Jul 23;15(1):45-49. doi: 10.1007/s12522-015-0214-8. eCollection 2016 Jan. Reprod Med Biol. 2015. PMID: 29259420 Free PMC article.
-
Cumulative live birth rates after one ART cycle including all subsequent frozen-thaw cycles in 1050 women: secondary outcome of an RCT comparing GnRH-antagonist and GnRH-agonist protocols.Hum Reprod. 2017 Mar 1;32(3):556-567. doi: 10.1093/humrep/dew358. Hum Reprod. 2017. PMID: 28130435 Clinical Trial.
-
Successful pregnancy and delivery after ovulation induction therapy in a woman with congenital hypogonadotropic hypogonadism: a case report.BMC Pregnancy Childbirth. 2023 May 11;23(1):338. doi: 10.1186/s12884-023-05682-7. BMC Pregnancy Childbirth. 2023. PMID: 37170100 Free PMC article.
-
Successful pregnancy and live birth despite discontinuation of hormone replacement therapy at 3 weeks and 5 days of gestation following vitrified-warmed embryo transfer under a hormone replacement therapy cycle: a case report and literature review.BMC Pregnancy Childbirth. 2024 Dec 20;24(1):831. doi: 10.1186/s12884-024-07059-w. BMC Pregnancy Childbirth. 2024. PMID: 39707226 Free PMC article. Review.
-
Live birth using vitrified--warmed oocytes in invasive ovarian cancer: case report and literature review.Reprod Biomed Online. 2014 Jun;28(6):663-8. doi: 10.1016/j.rbmo.2014.02.010. Epub 2014 Mar 4. Reprod Biomed Online. 2014. PMID: 24745835 Review.
References
-
- Bry-Gauillard H, Trabado S, Bouligand J, et al. Congenital hypogonadotropic hypogonadism in females: clinical spectrum, evaluation and genetics. Ann Endocrinol (Paris), 71: 158-162, 2010. - PubMed
-
- Cadman SM, Kim SH, Hu Y, Gonzalez-Martinez D, Bouloux PM. Molecular pathogenesis of Kallmann’s syndrome. Horm Res, 67: 231-242, 2007. - PubMed
-
- Young J, Xu C, Papadakis GE, et al. Clinical Management of Congenital Hypogonadotropic Hypogonadism. Endocr Rev, 40: 669-710, 2019. - PubMed
-
- Christou F, Pitteloud N, Gomez F. The induction of ovulation by pulsatile administration of GnRH: an appropriate method in hypothalamic amenorrhea. Gynecol Endocrinol, 33: 598-601, 2017. - PubMed