

Assessment of Aortoiliac Atherosclerotic Plaque on CT in Prostate Cancer Patients Undergoing Treatment
- PMID: 35314627
- PMCID: PMC8938817
- DOI: 10.3390/tomography8020050
Assessment of Aortoiliac Atherosclerotic Plaque on CT in Prostate Cancer Patients Undergoing Treatment
Abstract
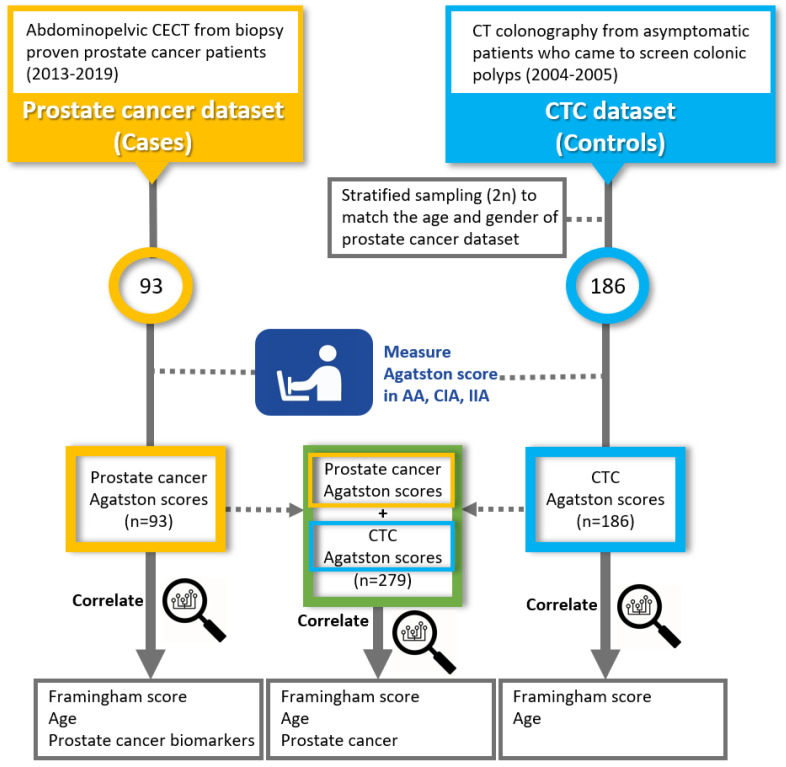
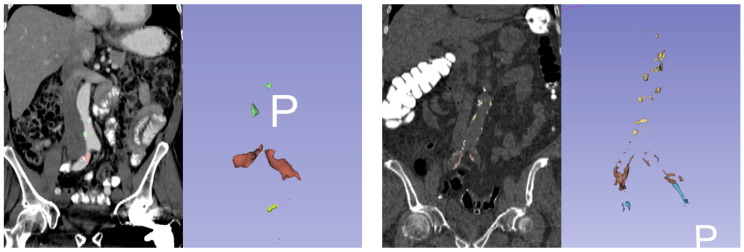
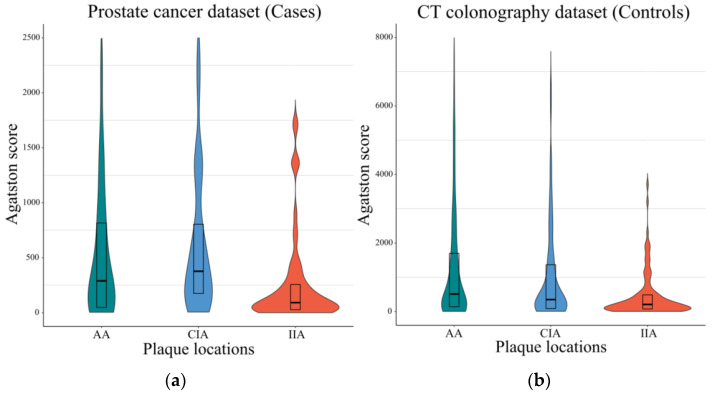
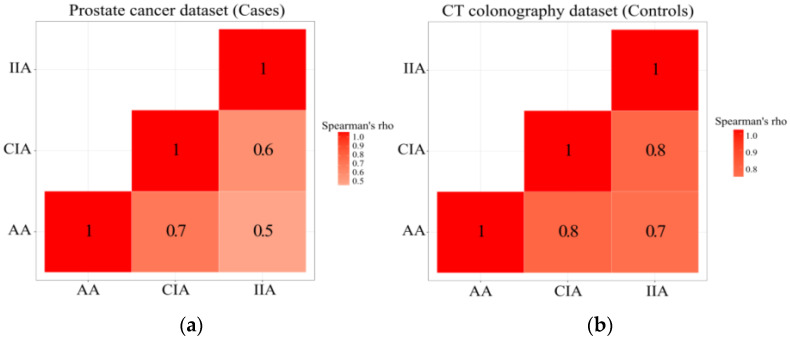
Traditionally, atherosclerotic risk factors for cardiovascular disease and cancer are assessed using coronary artery calcium scoring. However, this neglects the impact of atherosclerotic disease more proximal to the cancer site. This study assesses whether aortoiliac atherosclerotic plaque is associated with prostate cancer. The dataset consisted of abdominopelvic CT of 93 patients with prostate cancer and 186 asymptomatic patients who underwent CT colonography as an age- and gender-matched control group. Agatston scores were measured in the abdominal aorta, common iliac, and internal iliac arteries. The scores were evaluated for associations with age, Framingham risk score, and prostate cancer-related biomarkers, including prostate-specific antigen, Gleason score, tumor location, prostatectomy, androgen deprivation therapy, mortality, and bone metastasis. The atherosclerotic plaque of prostate cancer patients did not differ from the control group (p = 0.22) and was not correlated with any of the prostate cancer-related biomarkers (p > 0.05). However, Agatston scores of abdominal plaques correlated well with age (p < 0.001) and Framingham risk scores (p = 0.002).
Keywords: atherosclerotic plaques; cardiovascular diseases; contrast-enhanced; prostatic cancer.
Conflict of interest statement
Author P.J.P receives royalties from Elsevier. He holds stock/stock options in Elucent, Cellectar, and SHINE. He is a consultant for Bracco. His institution has grants/grants pending with the National Institutes of Health. Author R.M.S. receives royalties from iCAD, ScanMed, Philips, Translation Holdings, and Ping An. His lab received research support from Ping An.
Figures
Similar articles
-
Atherosclerotic Plaque Burden on Abdominal CT: Automated Assessment With Deep Learning on Noncontrast and Contrast-enhanced Scans.Acad Radiol. 2021 Nov;28(11):1491-1499. doi: 10.1016/j.acra.2020.08.022. Epub 2020 Sep 18. Acad Radiol. 2021. PMID: 32958429 Free PMC article.
-
CT attenuation features of individual calcified coronary plaque: differences among asymptomatic, stable angina pectoris, and acute coronary syndrome groups.PLoS One. 2015 Jun 24;10(6):e0131254. doi: 10.1371/journal.pone.0131254. eCollection 2015. PLoS One. 2015. PMID: 26106881 Free PMC article.
-
99mTc-MIP-1404 SPECT/CT for Assessment of Whole-Body Tumor Burden and Treatment Response in Patients With Biochemical Recurrence of Prostate Cancer.Clin Nucl Med. 2020 Aug;45(8):e349-e357. doi: 10.1097/RLU.0000000000003102. Clin Nucl Med. 2020. PMID: 32558706
-
Using clinical cardiovascular risk scores to predict coronary artery plaque severity and stenosis detected by CT coronary angiography in asymptomatic Chinese subjects.Int J Cardiovasc Imaging. 2011 Jun;27(5):669-78. doi: 10.1007/s10554-011-9874-6. Epub 2011 Jun 22. Int J Cardiovasc Imaging. 2011. PMID: 21695485
-
Extracoronary Thoracic and Coronary Artery Calcifications on Chest CT for Lung Cancer Screening: Association with Established Cardiovascular Risk Factors - The "CT-Risk" Trial.Acad Radiol. 2015 Jul;22(7):880-9. doi: 10.1016/j.acra.2015.03.005. Epub 2015 May 7. Acad Radiol. 2015. PMID: 25957500 Review.
Cited by
-
Progress in fully automated abdominal CT interpretation-an update over the past decade.Abdom Radiol (NY). 2025 Jul 8. doi: 10.1007/s00261-025-05094-5. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40627132 Review.
-
The Effect of Androgen Deprivation Therapy on the Cardiovascular System in Advanced Prostate Cancer.Medicina (Kaunas). 2024 Oct 22;60(11):1727. doi: 10.3390/medicina60111727. Medicina (Kaunas). 2024. PMID: 39596912 Free PMC article. Review.
References
-
- Whitlock M.C., Yeboah J., Burke G.L., Chen H., Klepin H.D., Hundley W.G. Cancer and Its Association With the Development of Coronary Artery Calcification: An Assessment From the Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2015;4:e002533. doi: 10.1161/JAHA.115.002533. - DOI - PMC - PubMed
-
- Thomas J.A., 2nd, Gerber L., Banez L.L., Moreira D.M., Rittmaster R.S., Andriole G.L., Freedland S.J. Prostate cancer risk in men with baseline history of coronary artery disease: Results from the REDUCE Study. Cancer Epidemiol. Biomark. Prev. 2012;21:576–581. doi: 10.1158/1055-9965.EPI-11-1017. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
