

CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions
- PMID: 35314628
- PMCID: PMC8938788
- DOI: 10.3390/tomography8020051
CT after Lung Microwave Ablation: Normal Findings and Evolution Patterns of Treated Lesions
Abstract
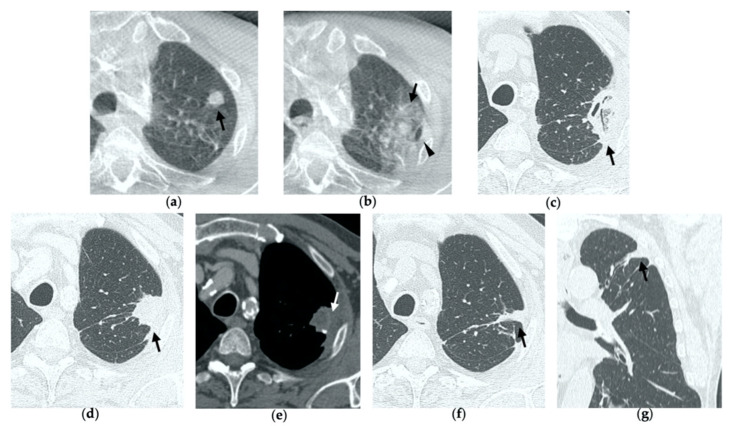
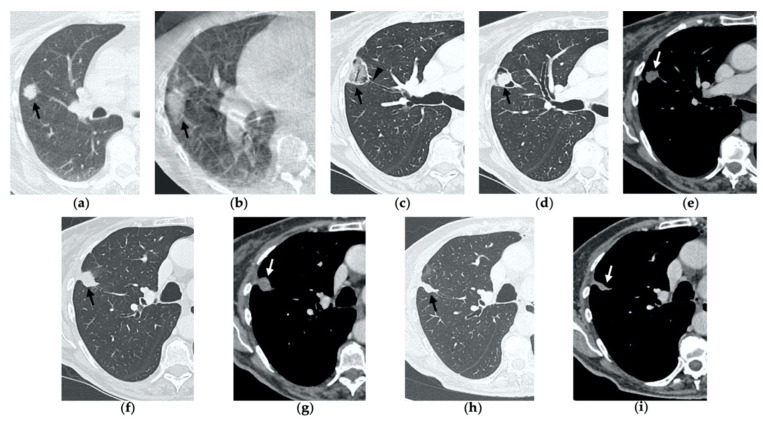
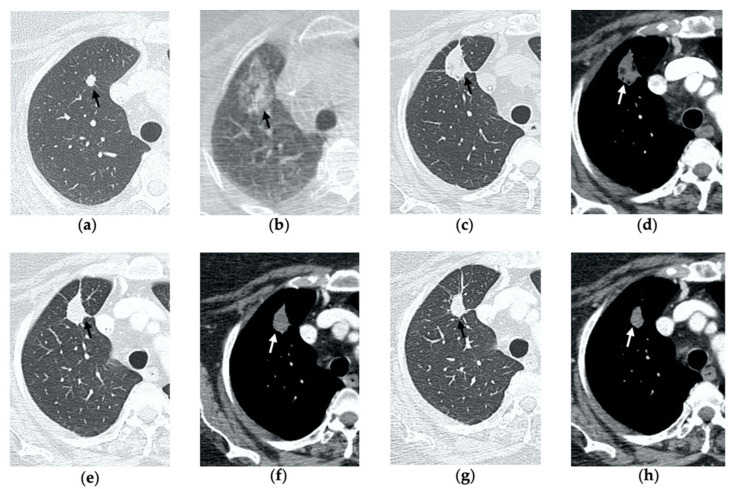
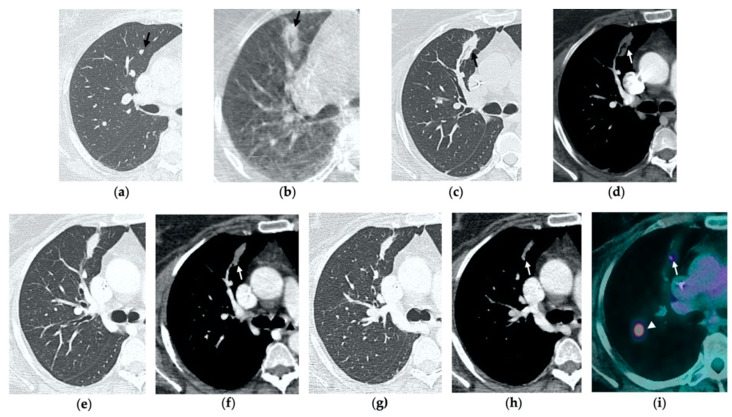
Imaging-guided percutaneous ablative treatments, such as radiofrequency ablation (RFA), cryoablation and microwave ablation (MWA), have been developed for the treatment of unresectable primary and secondary lung tumors in patients with advanced-stage disease or comorbidities contraindicating surgery. Among these therapies, MWA has recently shown promising results in the treatment of pulmonary neoplasms. The potential advantages of MWA over RFA include faster ablation times, higher intra-tumoral temperatures, larger ablation zones and lower susceptibility to the heat sink effect, resulting in greater efficacy in proximity to vascular structures. Despite encouraging results supporting its efficacy, there is a relative paucity of data in the literature regarding the role of computer tomography (CT) to monitor MWA-treated lesions, and the CT appearance of their morphologic evolution and complications. For both interventional and non-interventional radiologists, it is crucial to be familiar with the CT features of such treated lesions in order to detect incomplete therapy or recurrent disease at early stage, as well as to recognize initial signs of complications. The aim of this pictorial essay is to describe the typical CT features during follow-up of lung lesions treated with percutaneous MWA and how to interpret and differentiate them from other radiological findings, such as recurrence and complications, that are commonly encountered in this setting.
Keywords: CT; computed tomography; lung cancer; microwave ablation; percutaneous treatments.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Wang Y., Liu B., Cao P., Wang W., Wang W., Chang H., Li N., Li X., Zhao X., Li Y. Comparison between computed tomography-guided percutaneous microwave ablation and thoracoscopic lobectomy for stage I non-small cell lung cancer. Thorac. Cancer. 2018;9:1376–1382. doi: 10.1111/1759-7714.12842. - DOI - PMC - PubMed
-
- Kurilova I., Gonzalez-Aguirre A., Beets-Tan R.G., Erinjeri J., Petre E.N., Gonen M., Bains M., Kemeny N.E., Solomon S.B., Sofocleous C.T., et al. Microwave Ablation in the Management of Colorectal Cancer Pulmonary Metastases. Cardiovasc. Interv. Radiol. 2018;41:1530–1544. doi: 10.1007/s00270-018-2000-6. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
