

Early visual processing and adaptation as markers of disease, not vulnerability: EEG evidence from 22q11.2 deletion syndrome, a population at high risk for schizophrenia
- PMID: 35314711
- PMCID: PMC8938446
- DOI: 10.1038/s41537-022-00240-0
Early visual processing and adaptation as markers of disease, not vulnerability: EEG evidence from 22q11.2 deletion syndrome, a population at high risk for schizophrenia
Abstract
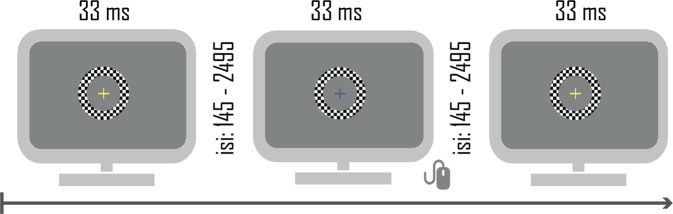
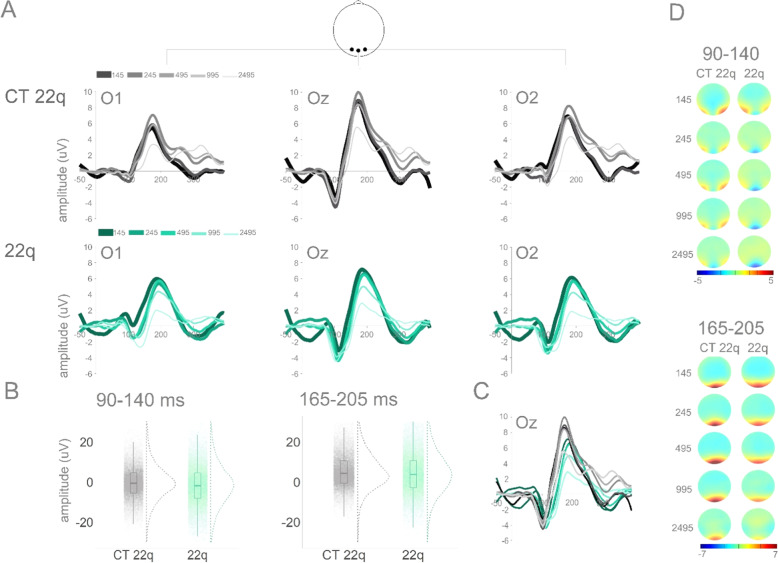
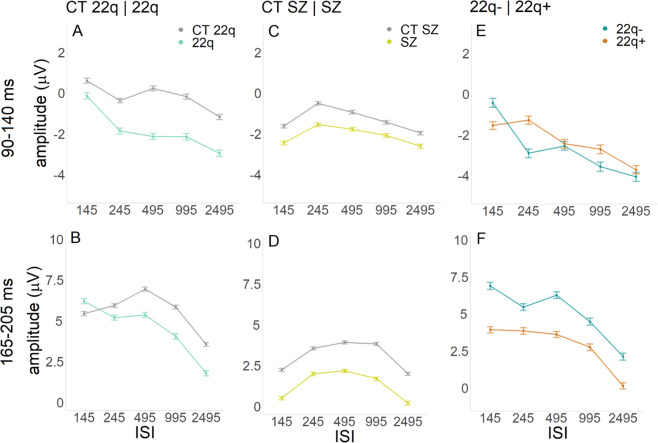
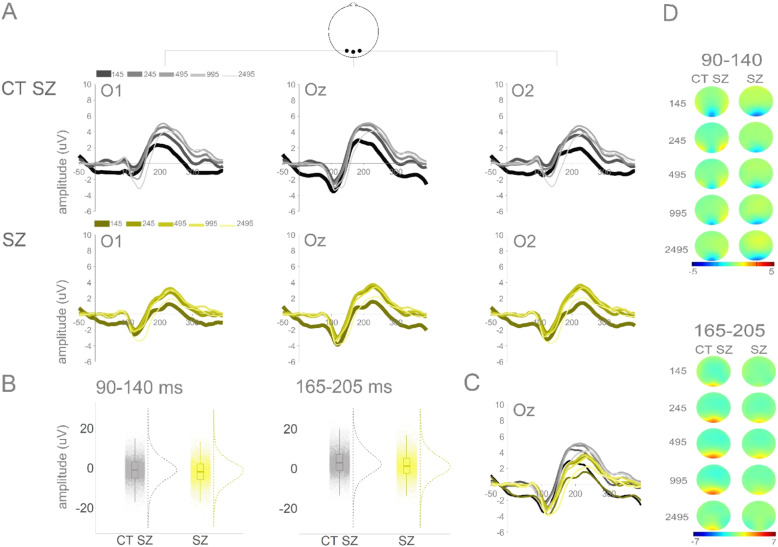
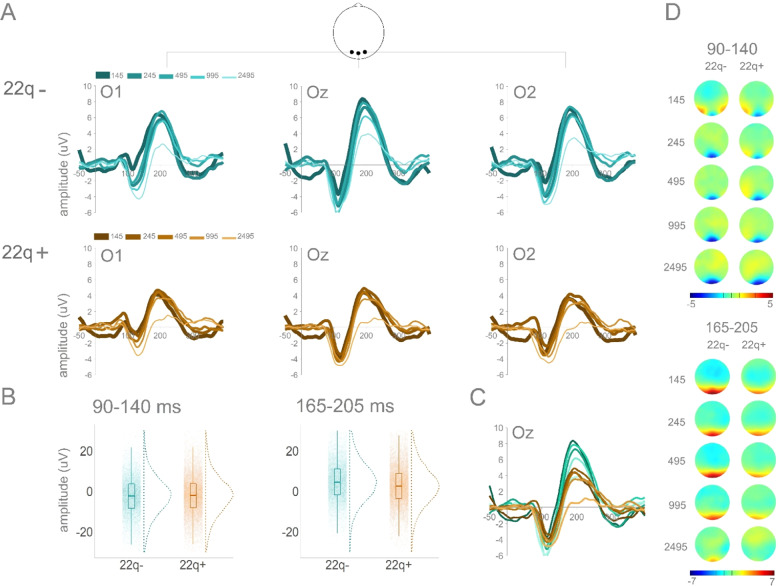
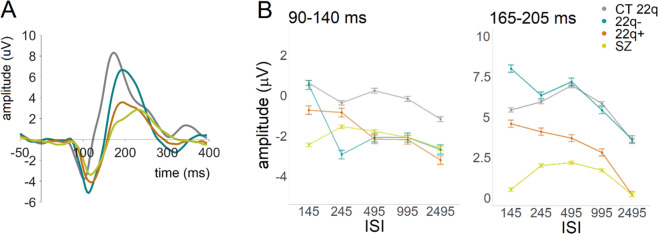
We investigated visual processing and adaptation in 22q11.2 deletion syndrome (22q11.2DS), a condition characterized by an increased risk for schizophrenia. Visual processing differences have been described in schizophrenia but remain understudied early in the disease course. Electrophysiology was recorded during a visual adaptation task with different interstimulus intervals to investigate visual processing and adaptation in 22q11.2DS (with (22q+) and without (22q-) psychotic symptoms), compared to control and idiopathic schizophrenia groups. Analyses focused on early windows of visual processing. While increased amplitudes were observed in 22q11.2DS in an earlier time window (90-140 ms), decreased responses were seen later (165-205 ms) in schizophrenia and 22q+. 22q11.2DS, and particularly 22q-, presented increased adaptation effects. We argue that while amplitude and adaptation in the earlier time window may reflect specific neurogenetic aspects associated with a deletion in chromosome 22, amplitude in the later window may be a marker of the presence of psychosis and/or of its chronicity/severity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Event-related potential (ERP) markers of 22q11.2 deletion syndrome and associated psychosis.J Neurodev Disord. 2023 Jun 16;15(1):19. doi: 10.1186/s11689-023-09487-9. J Neurodev Disord. 2023. PMID: 37328766 Free PMC article. Review.
-
Visual processing deficits in 22q11.2 Deletion Syndrome.Neuroimage Clin. 2017 Dec 21;17:976-986. doi: 10.1016/j.nicl.2017.12.028. eCollection 2018. Neuroimage Clin. 2017. PMID: 29527499 Free PMC article.
-
Atypical response inhibition and error processing in 22q11.2 Deletion Syndrome and schizophrenia: Towards neuromarkers of disease progression and risk.Neuroimage Clin. 2020;27:102351. doi: 10.1016/j.nicl.2020.102351. Epub 2020 Jul 17. Neuroimage Clin. 2020. PMID: 32731196 Free PMC article.
-
Assessing auditory processing endophenotypes associated with Schizophrenia in individuals with 22q11.2 deletion syndrome.Transl Psychiatry. 2020 Mar 5;10(1):85. doi: 10.1038/s41398-020-0764-3. Transl Psychiatry. 2020. PMID: 32139692 Free PMC article.
-
Update on the 22q11.2 deletion syndrome and its relevance to schizophrenia.Curr Opin Psychiatry. 2017 May;30(3):191-196. doi: 10.1097/YCO.0000000000000324. Curr Opin Psychiatry. 2017. PMID: 28230630 Review.
Cited by
-
Event-related potential (ERP) markers of 22q11.2 deletion syndrome and associated psychosis.J Neurodev Disord. 2023 Jun 16;15(1):19. doi: 10.1186/s11689-023-09487-9. J Neurodev Disord. 2023. PMID: 37328766 Free PMC article. Review.
-
Genetic modulation of brain dynamics in neurodevelopmental disorders: the impact of copy number variations on resting-state EEG.Transl Psychiatry. 2025 Apr 11;15(1):139. doi: 10.1038/s41398-025-03324-4. Transl Psychiatry. 2025. PMID: 40216767 Free PMC article.
References
-
- Baker KD, Skuse DH. Adolescents and young adults with 22qll deletion syndrome: psychopathology in an at-risk group. Br. J. Psychiatry. 2005;186:115–120. - PubMed
-
- Monks S, et al. Further evidence for high rates of schizophrenia in 22q11. 2 deletion syndrome. Schizophr. Res. 2014;153:231–236. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
