

Whole-genome risk prediction of common diseases in human preimplantation embryos
- PMID: 35314819
- PMCID: PMC8938270
- DOI: 10.1038/s41591-022-01735-0
Whole-genome risk prediction of common diseases in human preimplantation embryos
Abstract
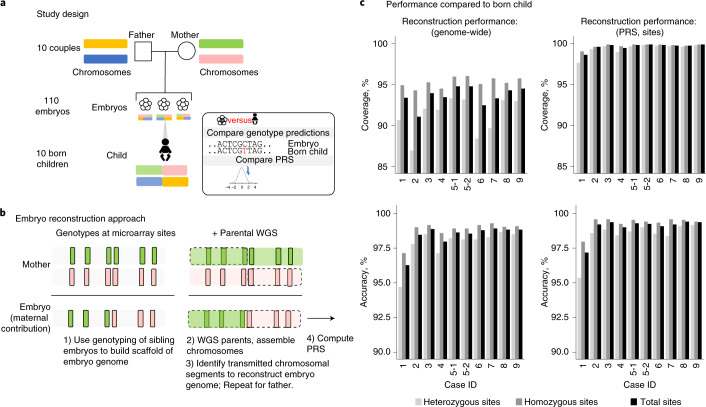
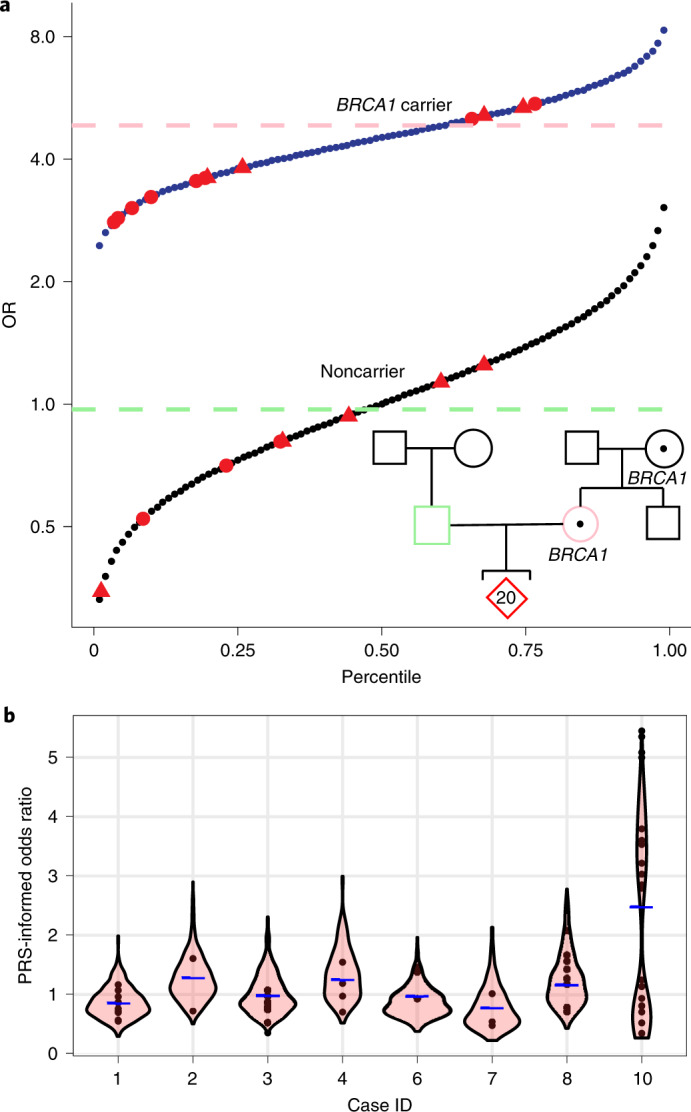
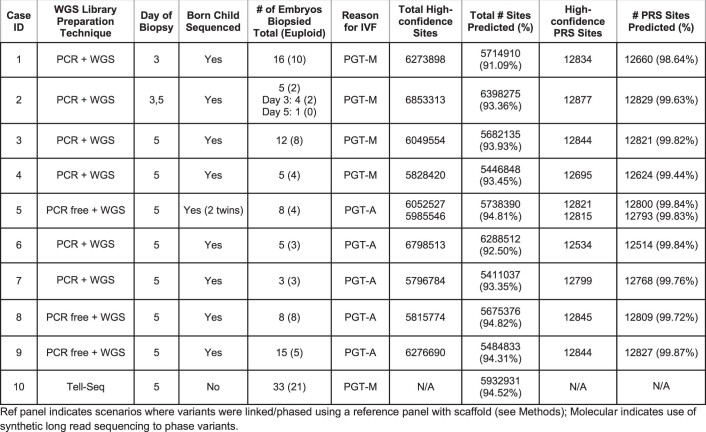
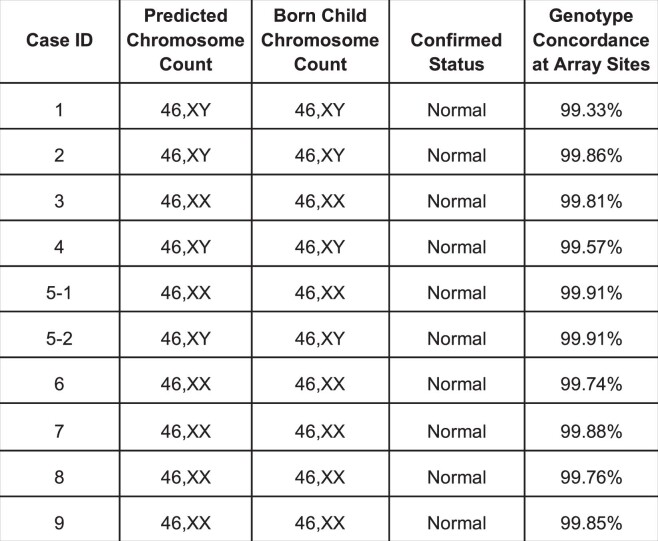
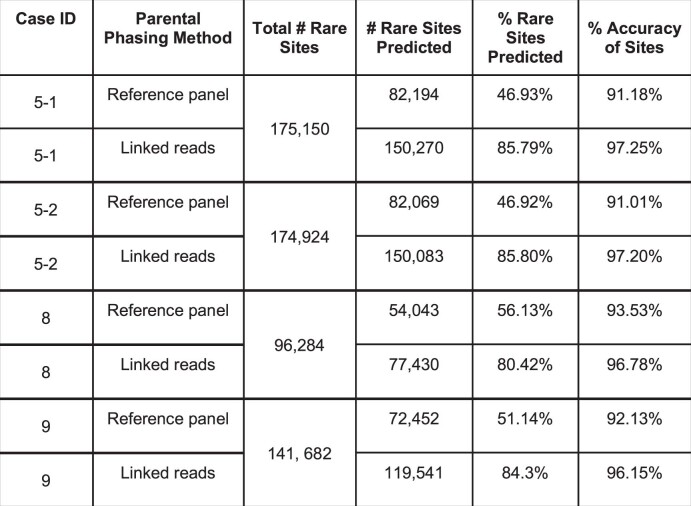
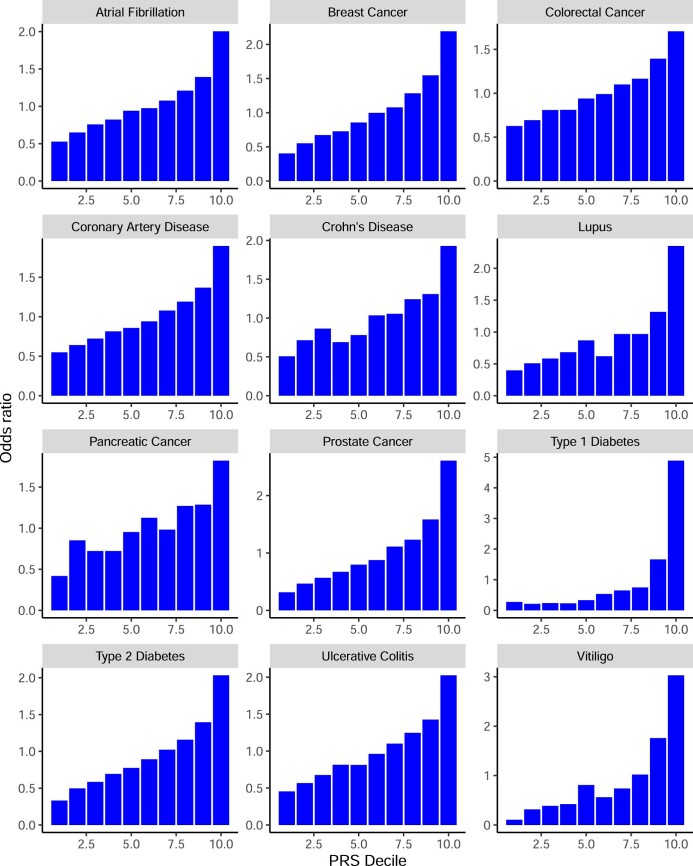
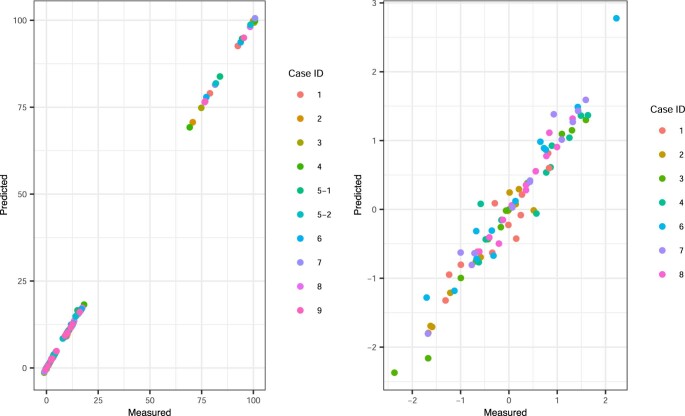
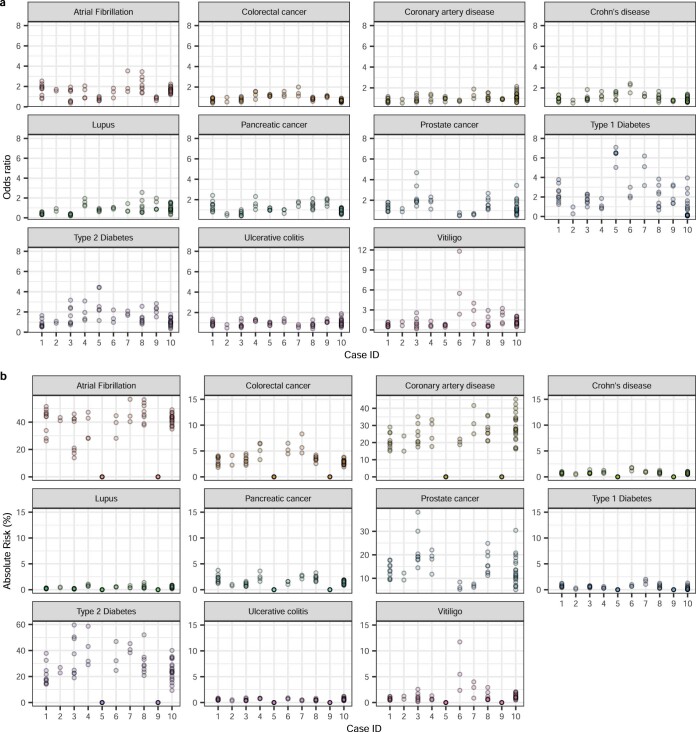
Preimplantation genetic testing (PGT) of in-vitro-fertilized embryos has been proposed as a method to reduce transmission of common disease; however, more comprehensive embryo genetic assessment, combining the effects of common variants and rare variants, remains unavailable. Here, we used a combination of molecular and statistical techniques to reliably infer inherited genome sequence in 110 embryos and model susceptibility across 12 common conditions. We observed a genotype accuracy of 99.0-99.4% at sites relevant to polygenic risk scoring in cases from day-5 embryo biopsies and 97.2-99.1% in cases from day-3 embryo biopsies. Combining rare variants with polygenic risk score (PRS) magnifies predicted differences across sibling embryos. For example, in a couple with a pathogenic BRCA1 variant, we predicted a 15-fold difference in odds ratio (OR) across siblings when combining versus a 4.5-fold or 3-fold difference with BRCA1 or PRS alone. Our findings may inform the discussion of utility and implementation of genome-based PGT in clinical practice.
© 2022. The Author(s).
Conflict of interest statement
A.K., K.I., J.S., O.S., T.T., D.H. and M.R. are either current or previous employees of, and M.B., G.G., P.C.N., B.L. and L.G. are either current or previous consultants with, MyOme. M.R., D.K., M.B. and M.K. are current employees of Natera. The remaining authors declare no competing interests.
Figures
Comment in
-
Polygenic embryo testing: understated ethics, unclear utility.Nat Med. 2022 Mar;28(3):446-448. doi: 10.1038/s41591-022-01743-0. Nat Med. 2022. PMID: 35314818 Free PMC article.
-
The alarming rise of complex genetic testing in human embryo selection.Nature. 2022 Mar;603(7902):549-550. doi: 10.1038/d41586-022-00787-z. Nature. 2022. PMID: 35314828 No abstract available.
References
-
- Handyside AH, et al. Validation and first clinical application of karyomapping for preimplantation diagnosis (PGD) of Gaucher disease combined with 24 chromosome screening. Fertil. Steril. 2010;94:S79–S80. doi: 10.1016/j.fertnstert.2010.07.309. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
