

Diagnostic variation for febrile children in European emergency departments
- PMID: 35314869
- PMCID: PMC9110537
- DOI: 10.1007/s00431-022-04417-8
Diagnostic variation for febrile children in European emergency departments
Abstract
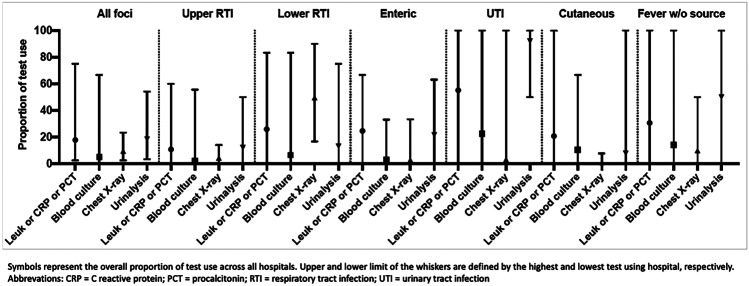
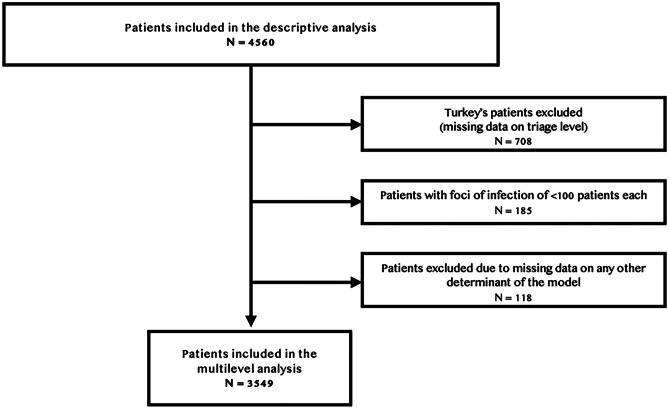
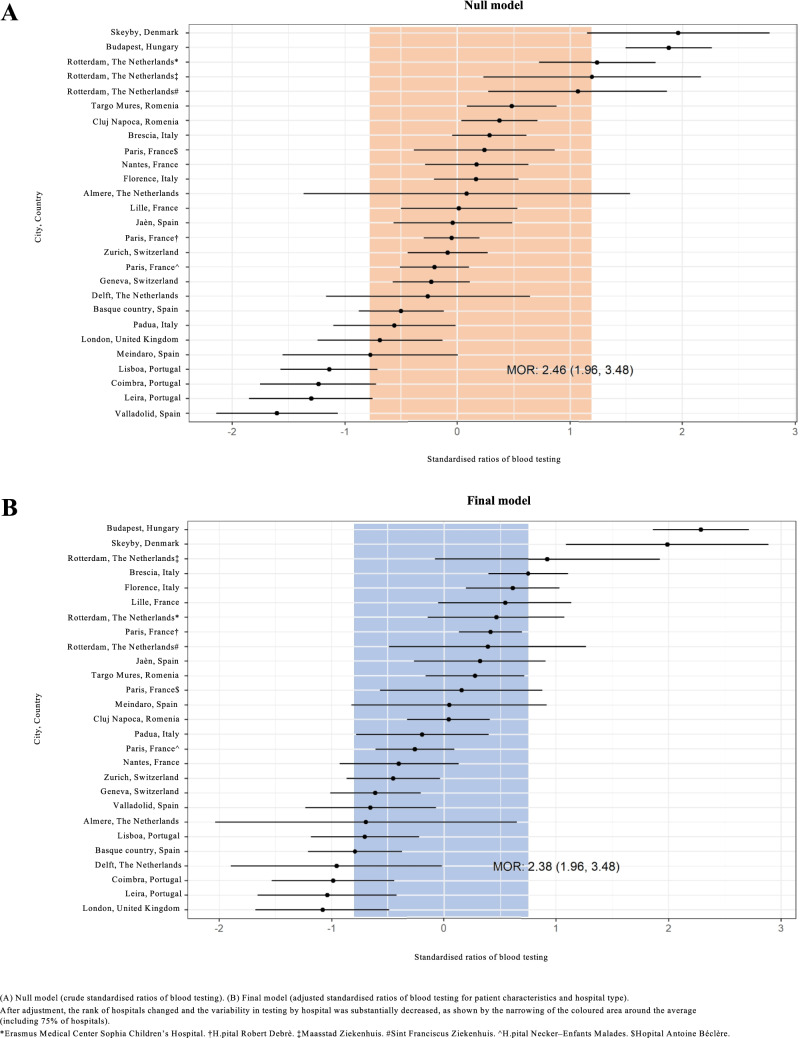
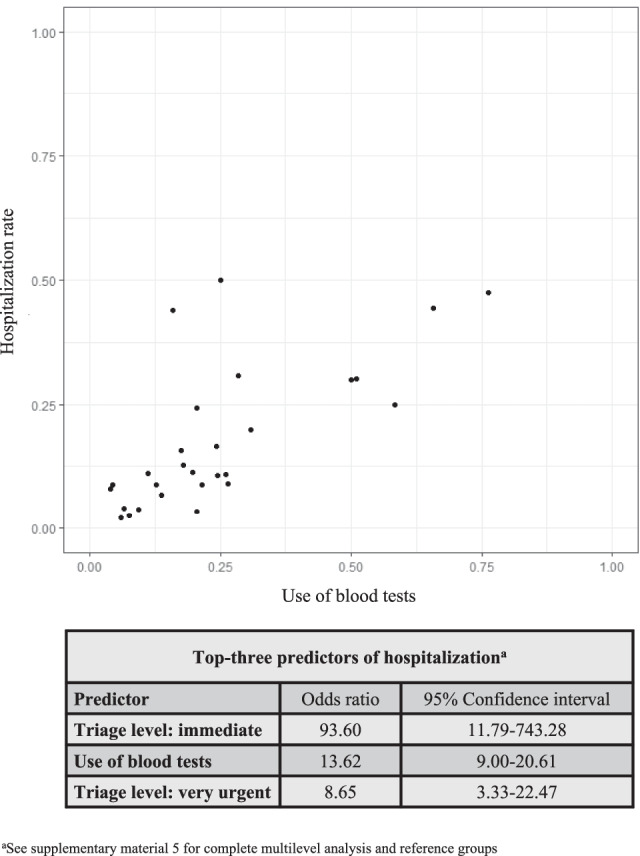
The study aimed to explore the use of diagnostics for febrile children presenting to European emergency departments (EDs), the determinants of inter-hospital variation, and the association between test use and hospitalization. We performed a secondary analysis of a cross-sectional observational study involving 28 paediatric EDs from 11 countries. A total of 4560 children < 16 years were included, with fever as reason for consultation. We excluded neonates and children with relevant comorbidities. Our primary outcome was the proportion of children receiving testing after primary evaluation, by country and by focus of infection. Variability between hospitals and effects of blood testing on patient disposition were explored by multilevel regression analyses, adjusting for patient characteristics (age group, triage level, appearance, fever duration, focus of infection) and hospital type (academic, teaching, other). The use of routine diagnostics varied widely, mostly in the use of blood tests, ranging from 3 to 75% overall across hospitals. Age < 3 months, high-acuity triage level, ill appearance, and suspicion of urinary tract infection displayed the strongest association with blood testing (odds ratios (OR) of 8.71 (95% CI 5.23-14.53), 19.46 (3.66-103.60), 3.13 (2.29-4.26), 10.84 (6.35-18.50), respectively). Blood testing remained highly variable across hospitals (median OR of the final model 2.36, 1.98-3.54). A positive association was observed between blood testing and hospitalization (OR 13.62, 9.00-20.61).
Conclusion: the use of diagnostics for febrile children was highly variable across European EDs, yet patient and hospital characteristics could only partly explain inter-hospital variability. Focus groups of participating sites should help define reasons for unexpected variation.
What is known: • Although previous research has shown variation in the emergency department (ED) management of febrile children, there is limited information on the use of diagnostics in European EDs. • A deeper knowledge of variability and its determinants can steer optimization of care.
What is new: • The use of diagnostics for febrile children was highly variable across European EDs, yet patient and hospital characteristics could only partly explain inter-hospital variability. • Data on between-centre comparison offer opportunities to further explore factors influencing unwarranted variation.
Keywords: Blood testing; Children; Diagnosis; Emergency department; Fever; Variation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Craig JC, Williams GJ, Jones M, Codarini M, Macaskill P, Hayen A, Irwig L, Fitzgerald DA, Isaacs D, McCaskill M. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. BMJ. 2010;340:c1594. doi: 10.1136/bmj.c1594. - DOI - PMC - PubMed
-
- Nijman RG, Vergouwe Y, Thompson M, van Veen M, van Meurs AH, van der Lei J, Steyerberg EW, Moll HA, Oostenbrink R. Clinical prediction model to aid emergency doctors managing febrile children at risk of serious bacterial infections: diagnostic study. BMJ. 2013;346:f1706. doi: 10.1136/bmj.f1706. - DOI - PMC - PubMed
-
- Irwin AD, Grant A, Williams R, Kolamunnage-Dona R, Drew RJ, Paulus S, Jeffers G, Williams K, Breen R, Preston J, Appelbe D, Chesters C, Newland P, Marzouk O, McNamara PS, Diggle PJ, Carrol ED (2017) Predicting risk of serious bacterial infections in febrile children in the emergency department. Pediatrics 140(2). 10.1542/peds.2016-2853 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
