

Impact of omitting fluorouracil from FOLFIRI plus bevacizumab as second-line chemotherapy for patients with metastatic colorectal cancer
- PMID: 35314873
- PMCID: PMC11796750
- DOI: 10.1007/s00432-022-03979-2
Impact of omitting fluorouracil from FOLFIRI plus bevacizumab as second-line chemotherapy for patients with metastatic colorectal cancer
Abstract
Purpose: Fluorouracil, leucovorin, and irinotecan (FOLFIRI) plus bevacizumab is the standard second-line chemotherapy for patients with metastatic colorectal cancer (mCRC) who are refractory or intolerant to fluoropyrimidines and oxaliplatin. However, the benefits of incorporating fluoropyrimidines into second-line chemotherapy for patients with mCRC who are refractory to fluoropyrimidines are unknown.
Methods: We retrospectively evaluated patients with mCRC who were administered irinotecan plus bevacizumab or FOLFIRI plus bevacizumab as second-line chemotherapy at a single institution from January 2010 to April 2020. We compared the efficacy and safety of irinotecan plus bevacizumab (IRI group) with those of FOLFIRI plus bevacizumab (FOLFIRI group).
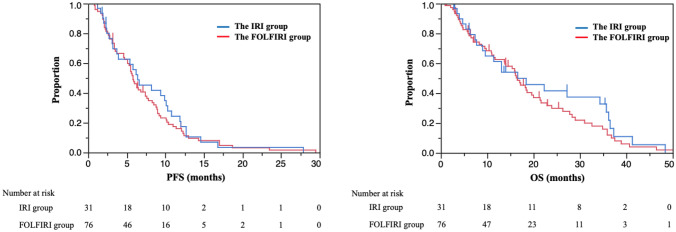
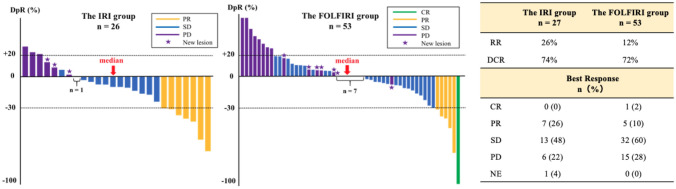
Results: Of the 255 enrolled patients, 107 (IRI/FOLFIRI group, 31/76 patients) were eligible for analysis. After a median follow-up of 13.1 months (range 1.2-48.4) and 14.3 months (range 0.9-46.5) for the IRI and FOLFIRI groups, respectively, the median progression-free survival was 6.4 months and 5.8 months [adjusted hazard ratio (aHR), 0.82; 95% confidence interval (CI) 0.50-1.34, p = 0.44] and the median overall survival was 16.6 months and 16.5 months (aHR, 1.01; 95% CI 0.59-1.69; p = 0.97) in the IRI and FOLFIRI groups, respectively. All-grade nausea, stomatitis, neutropenia, thrombocytopenia, Grade 3/4 neutropenia, and febrile neutropenia occurred more frequently in the FOLFIRI group than in the IRI group.
Conclusion: Our study suggests omitting fluorouracil from FOLFIRI plus bevacizumab as the second-line chemotherapy decreases adverse events without affecting the treatment efficacy in patients with mCRC who are refractory to fluoropyrimidines. Further randomized prospective studies are warranted to validate our result.
Keywords: Bevacizumab; Chemotherapy; Colorectal cancer; Fluoropyrimidine; Irinotecan.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
The authors declare the following conflicts of interest: YM received honorania from Takeda, Merck Bio Pharma, and Taiho. TM received honorania from Takeda, Chudai, Merck Bio Pharma, Taiho, Bayer, Eli Lilly, Yakult Honsha, Sanofi, Daiichi Sankyo, Ono, and Bristol-myers squibb and research funding from MSD, Daiichi Sankyo, Ono, and Novartis. TO received honorania from Ono, Bristol-myers squibb, Taiho, MSD, and Eli Lilly. TN received honorania from Eli Lilly. YN received honorania from Yakult Honsha, Taiho, Eli Lilly, Daiichi Sankyo, and AstraZeneca and research funding from Ono, and Bristol-myers squibb. YN was also a part of the advisory board of Daiichi Sankyo. HB received honorania from Eli Lilly and Taiho and research funding from Ono. HT received honorania from Taiho, Chugai, Takeda, Eli Lilly, Merck Biopharma, and Yakult Honsha. SK received honorania from Bristol-myers squibb, Chugai, Merck Bio Pharma, Daiichi Sankyo, MSD, Ono, Bayer, Taiho, and Esai and research funding from Ono, Taiho, MSD, Nobelpharma, Bristol-myers squibb, Eli Lilly, and Chugai. MT received honorania from EA Pharma. KM received honorania from Ono, Chugai, Takeda, Taiho, Sanofi, Bristol-myers squibb, Eli Lilly, and Bayer; research funding from Solasia Pharma, Merck Serono, Daiichi Sankyo, Parexel International, Pfizer, MSD, Amgen, ONO, Astellas, Sanofi, Taiho, and Esai; and consulting fees from AstraZeneca, Ono, and Amgen. KM was also a part of the advisory boards of Ono, MSD, AstraZeneca, Daiichi Sankyo, and Solasia Pharma.
Figures
Similar articles
-
Irinotecan chemotherapy combined with fluoropyrimidines versus irinotecan alone for overall survival and progression-free survival in patients with advanced and/or metastatic colorectal cancer.Cochrane Database Syst Rev. 2016 Feb 12;2(2):CD008593. doi: 10.1002/14651858.CD008593.pub3. Cochrane Database Syst Rev. 2016. PMID: 26869023 Free PMC article.
-
Real-World Analysis of Irinotecan With or Without Fluorouracil in the Second-Line Treatment of Metastatic Colorectal Cancer.J Natl Compr Canc Netw. 2025 Aug;23(8):e257031. doi: 10.6004/jnccn.2025.7031. J Natl Compr Canc Netw. 2025. PMID: 40763782
-
Second-line systemic therapy for metastatic colorectal cancer.Cochrane Database Syst Rev. 2017 Jan 27;1(1):CD006875. doi: 10.1002/14651858.CD006875.pub3. Cochrane Database Syst Rev. 2017. PMID: 28128439 Free PMC article.
-
FOLFIRINOX-3 plus bevacizumab (bFOLFIRINOX3) in chemo-refractory metastatic colorectal cancer: a multicenter phase II trial.Future Oncol. 2025 Mar;21(6):699-706. doi: 10.1080/14796694.2025.2461446. Epub 2025 Feb 6. Future Oncol. 2025. PMID: 39913183 Free PMC article. Clinical Trial.
-
Modified FOLFOX6 plus bevacizumab with and without nivolumab for first-line treatment of metastatic colorectal cancer: phase 2 results from the CheckMate 9X8 randomized clinical trial.J Immunother Cancer. 2024 Mar 13;12(3):e008409. doi: 10.1136/jitc-2023-008409. J Immunother Cancer. 2024. PMID: 38485190 Free PMC article. Clinical Trial.
References
-
- Ando Y, Saka H, Ando M, Sawa T, Muro K, Ueoka H, Yokoyama A, Saitoh S, Shimokata K, Hasegawa Y (2000) Polymorphisms of UDP-glucuronosyltransferase gene and irinotecan toxicity: a pharmacogenetic analysis. Cancer Res 60(24):6921–6926 - PubMed
-
- Becouarn Y, Gamelin E, Coudert B, Négrier S, Pierga JY, Raoul JL, Provençal J, Rixe O, Krisch C, Germa C, Bekradda M, Mignard D, Mousseau M (2001) Randomized multicenter phase II study comparing a combination of fluorouracil and folinic acid and alternating irinotecan and oxaliplatin with oxaliplatin and irinotecan in fluorouracil-pretreated metastatic colorectal cancer patients. J Clin Oncol 19(22):4195–4201 - PubMed
-
- Clarke SJ, Yip S, Brown C, van Hazel GA, Ransom DT, Goldstein D, Jeffrey GM, Tebbutt NC, Buck M, Lowenthal RM, Boland A, Gebski V, Zalcberg J, Simes RJ (2011) Single-agent irinotecan or FOLFIRI as second-line chemotherapy for advanced colorectal cancer; results of a randomised phase II study (DaVINCI) and meta-analysis [corrected]. Eur J Cancer 47(12):1826–1836 - PubMed
-
- Graeven U, Arnold D, Reinacher-Schick A, Heuer T, Nusch A, Porschen R, Schmiegel W (2007) A randomised phase II study of irinotecan in combination with 5-FU/FA compared with irinotecan alone as second-line treatment of patients with metastatic colorectal carcinoma. Onkologie 30(4):169–174 - PubMed
-
- Kayhanian H, Goode E, Sclafani F, Ang JE, Gerlinger M, Gonzalez de Castro D, Shepherd S, Peckitt C, Rao S, Watkins D, Chau I, Cunningham D, Starling N (2018) Treatment and survival outcome of BRAF-mutated metastatic colorectal cancer: a retrospective matched case-control study. Clin Colorect Cancer 17(1):e69–e76 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
