

Liver Venous Deprivation (LVD) Versus Portal Vein Embolization (PVE) Alone Prior to Extended Hepatectomy: A Matched Pair Analysis
- PMID: 35314879
- PMCID: PMC9226084
- DOI: 10.1007/s00270-022-03107-0
Liver Venous Deprivation (LVD) Versus Portal Vein Embolization (PVE) Alone Prior to Extended Hepatectomy: A Matched Pair Analysis
Abstract
Background: To investigate whether liver venous deprivation (LVD) as simultaneous, portal vein (PVE) and right hepatic vein embolization offers advantages in terms of hypertrophy induction before extended hepatectomy in non-cirrhotic liver.
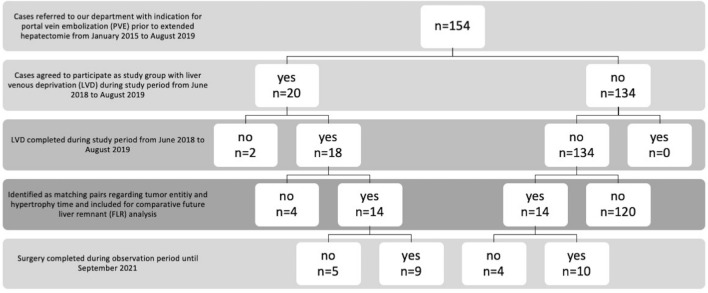
Materials and methods: Between June 2018 and August 2019, 20 patients were recruited for a prospective, non-randomized study to investigate the efficacy of LVD. After screening of 134 patients treated using PVE alone from January 2015 to August 2019, 14 directly matched pairs regarding tumor entity (cholangiocarcinoma, CC and colorectal carcinoma, CRC) and hypertrophy time (defined as time from embolization to follow-up imaging) were identified. In both treatment groups, the same experienced reader (> 5 years experience) performed imaging-based measurement of the volumes of liver segments of the future liver remnant (FLR) prior to embolization and after the standard clinical hypertrophy interval (~ 30 days), before surgery. Percentage growth of segments was calculated and compared.
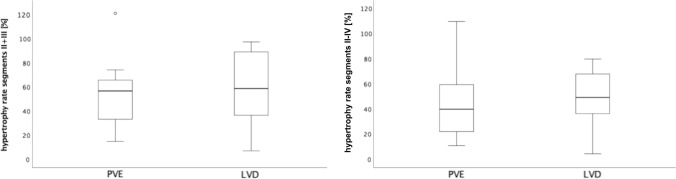
Results: After matched follow-up periods (mean of 30.5 days), there were no statistically significant differences in relative hypertrophy of FLRs. Mean ± standard deviation relative hypertrophy rates for LVD/PVE were 59 ± 29.6%/54.1 ± 27.6% (p = 0.637) for segments II + III and 48.2 ± 22.2%/44.9 ± 28.9% (p = 0.719) for segments II-IV, respectively.
Conclusions: LVD had no significant advantages over the standard method (PVE alone) in terms of hypertrophy induction of the FLR before extended hepatectomy in this study population.
Keywords: Extended hepatectomy; Future liver remnant (FLR); Liver venous deprivation (LVD); Portal vein embolization (PVE); Right hepatic vein embolization (rHVE).
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
Comment in
-
Liver Venous Deprivation Versus Portal Vein Embolization: Are We Really Comparing Like with Like?Cardiovasc Intervent Radiol. 2022 Dec;45(12):1888-1889. doi: 10.1007/s00270-022-03263-3. Epub 2022 Sep 8. Cardiovasc Intervent Radiol. 2022. PMID: 36076108 No abstract available.
Similar articles
-
Propensity Score-Matched Analysis of Liver Venous Deprivation and Portal Vein Embolization Before Planned Hepatectomy in Patients with Extensive Colorectal Liver Metastases and High-Risk Factors for Inadequate Regeneration.Ann Surg Oncol. 2025 Mar;32(3):1752-1761. doi: 10.1245/s10434-024-16558-1. Epub 2024 Dec 4. Ann Surg Oncol. 2025. PMID: 39633174
-
Simultaneous portal and hepatic vein embolization is better than portal embolization or ALPPS for hypertrophy of future liver remnant before major hepatectomy: A systematic review and network meta-analysis.Hepatobiliary Pancreat Dis Int. 2023 Jun;22(3):221-227. doi: 10.1016/j.hbpd.2022.08.013. Epub 2022 Sep 7. Hepatobiliary Pancreat Dis Int. 2023. PMID: 36100542
-
Study protocol of the HYPER-LIV01 trial: a multicenter phase II, prospective and randomized study comparing simultaneous portal and hepatic vein embolization to portal vein embolization for hypertrophy of the future liver remnant before major hepatectomy for colo-rectal liver metastases.BMC Cancer. 2020 Jun 19;20(1):574. doi: 10.1186/s12885-020-07065-z. BMC Cancer. 2020. PMID: 32560632 Free PMC article.
-
Hepatic vein embolization after portal vein embolization to induce additional liver hypertrophy in patients with metastatic colorectal carcinoma.Eur Radiol. 2020 Jul;30(7):3862-3868. doi: 10.1007/s00330-020-06746-4. Epub 2020 Mar 7. Eur Radiol. 2020. PMID: 32144462
-
Comparison of liver venous deprivation with portal vein embolization alone in patients undergoing major liver resection: a systematic review and meta-analysis.HPB (Oxford). 2024 Nov;26(11):1329-1338. doi: 10.1016/j.hpb.2024.07.409. Epub 2024 Jul 16. HPB (Oxford). 2024. PMID: 39054212
Cited by
-
A systematic review and meta-analysis of liver venous deprivation versus portal vein embolization before hepatectomy: future liver volume, postoperative outcomes, and oncological safety.Front Med (Lausanne). 2024 Jan 10;10:1334661. doi: 10.3389/fmed.2023.1334661. eCollection 2023. Front Med (Lausanne). 2024. PMID: 38269320 Free PMC article.
-
Propensity Score-Matched Analysis of Liver Venous Deprivation and Portal Vein Embolization Before Planned Hepatectomy in Patients with Extensive Colorectal Liver Metastases and High-Risk Factors for Inadequate Regeneration.Ann Surg Oncol. 2025 Mar;32(3):1752-1761. doi: 10.1245/s10434-024-16558-1. Epub 2024 Dec 4. Ann Surg Oncol. 2025. PMID: 39633174
-
Multi-organ Radiomics-Based Prediction of Future Remnant Liver Hypertrophy Following Portal Vein Embolization.Ann Surg Oncol. 2023 Dec;30(13):7976-7985. doi: 10.1245/s10434-023-14241-5. Epub 2023 Sep 5. Ann Surg Oncol. 2023. PMID: 37670120 Free PMC article.
-
CIRSE Standards of Practice on Portal Vein Embolization and Double Vein Embolization/Liver Venous Deprivation.Cardiovasc Intervent Radiol. 2024 Aug;47(8):1025-1036. doi: 10.1007/s00270-024-03743-8. Epub 2024 Jun 17. Cardiovasc Intervent Radiol. 2024. PMID: 38884781 Free PMC article.
-
Locoregional Therapy in the Management of Intrahepatic Cholangiocarcinoma: Is There Sufficient Evidence to Guide Current Clinical Practice?Curr Oncol Rep. 2022 Dec;24(12):1741-1750. doi: 10.1007/s11912-022-01338-5. Epub 2022 Oct 18. Curr Oncol Rep. 2022. PMID: 36255606 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
