

Complement C4 Copy Number Variation is Linked to SSA/Ro and SSB/La Autoantibodies in Systemic Inflammatory Autoimmune Diseases
- PMID: 35315244
- PMCID: PMC9543510
- DOI: 10.1002/art.42122
Complement C4 Copy Number Variation is Linked to SSA/Ro and SSB/La Autoantibodies in Systemic Inflammatory Autoimmune Diseases
Abstract
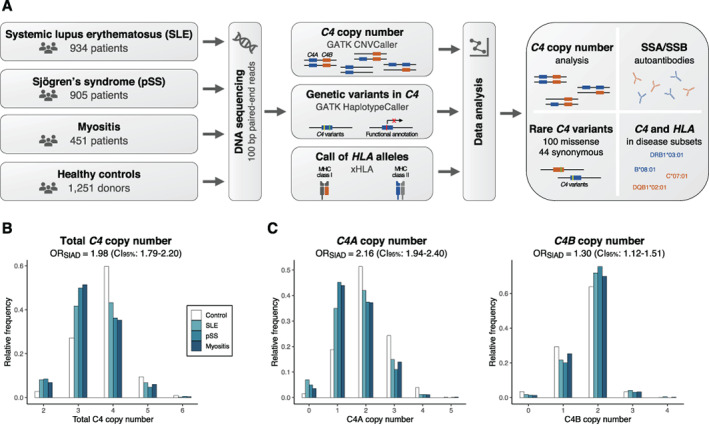
Objective: Copy number variation of the C4 complement components, C4A and C4B, has been associated with systemic inflammatory autoimmune diseases. This study was undertaken to investigate whether C4 copy number variation is connected to the autoimmune repertoire in systemic lupus erythematosus (SLE), primary Sjögren's syndrome (SS), or myositis.
Methods: Using targeted DNA sequencing, we determined the copy number and genetic variants of C4 in 2,290 well-characterized Scandinavian patients with SLE, primary SS, or myositis and 1,251 healthy controls.
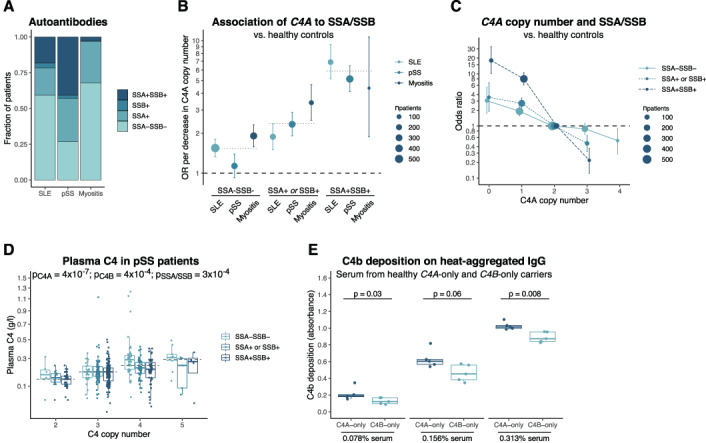
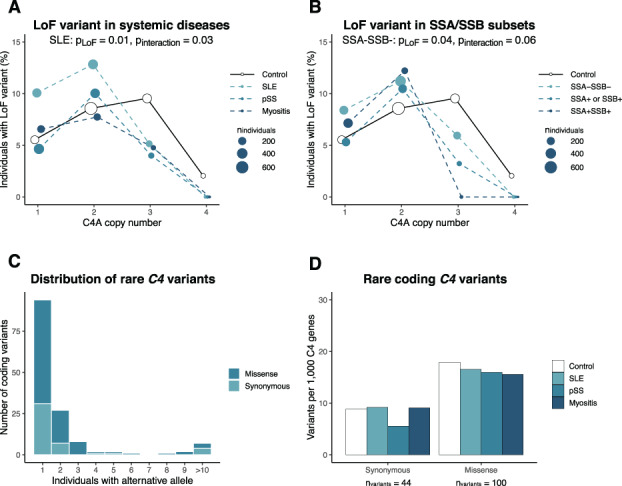
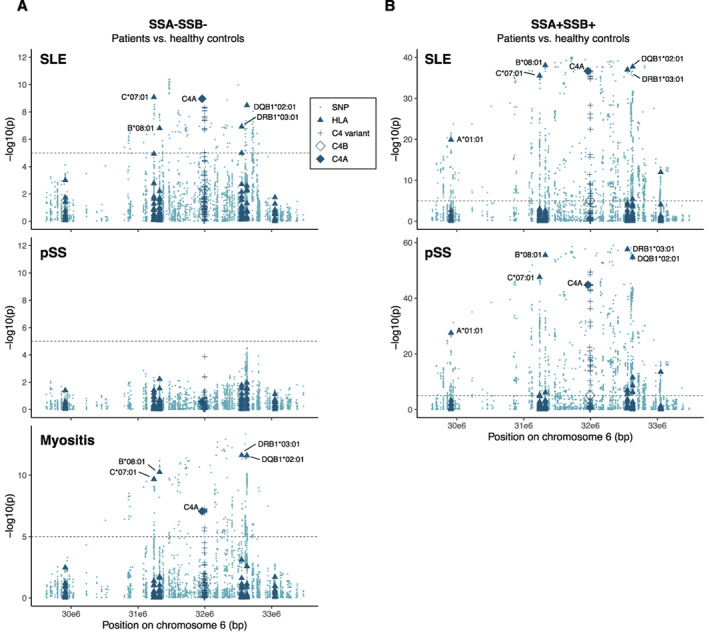
Results: A prominent relationship was observed between C4A copy number and the presence of SSA/SSB autoantibodies, which was shared between the 3 diseases. The strongest association was detected in patients with autoantibodies against both SSA and SSB and 0 C4A copies when compared to healthy controls (odds ratio [OR] 18.0 [95% confidence interval (95% CI) 10.2-33.3]), whereas a weaker association was seen in patients without SSA/SSB autoantibodies (OR 3.1 [95% CI 1.7-5.5]). The copy number of C4 correlated positively with C4 plasma levels. Further, a common loss-of-function variant in C4A leading to reduced plasma C4 was more prevalent in SLE patients with a low copy number of C4A. Functionally, we showed that absence of C4A reduced the individuals' capacity to deposit C4b on immune complexes.
Conclusion: We show that a low C4A copy number is more strongly associated with the autoantibody repertoire than with the clinically defined disease entities. These findings may have implications for understanding the etiopathogenetic mechanisms of systemic inflammatory autoimmune diseases and for patient stratification when taking the genetic profile into account.
© 2022 The Authors. Arthritis & Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures
Comment in
-
C4A copy number is associated with autoimmune disease.Nat Rev Rheumatol. 2022 May;18(5):246. doi: 10.1038/s41584-022-00781-9. Nat Rev Rheumatol. 2022. PMID: 35383316 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
