

Midline Brain Shift After Hemispheric Surgery: Natural History, Clinical Significance, and Association With Cerebrospinal Fluid Diversion
- PMID: 35315814
- PMCID: PMC9514754
- DOI: 10.1227/ons.0000000000000134
Midline Brain Shift After Hemispheric Surgery: Natural History, Clinical Significance, and Association With Cerebrospinal Fluid Diversion
Abstract
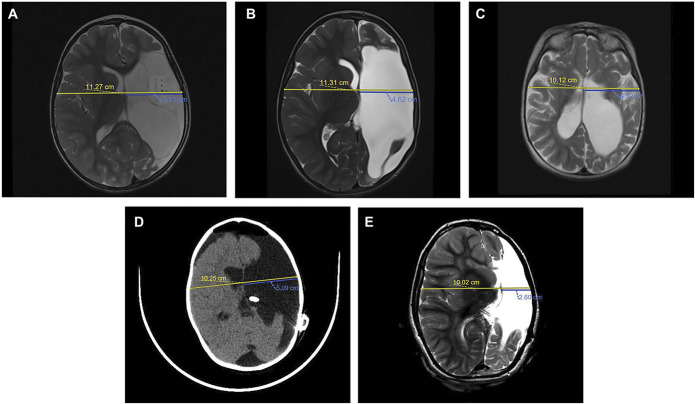
Background: Hemispherectomy and its modern variants are effective surgical treatments for medically intractable unihemispheric epilepsy. Although some complications such as posthemispherectomy hydrocephalus are well documented, midline brain shift (MLBS) after hemispheric surgery has only been described anecdotally and never formally studied.
Objective: To assess the natural history and clinical relevance of MLBS and determine whether cerebrospinal fluid (CSF) shunting of the ipsilateral surgical cavity exacerbates MLBS posthemispheric surgery.
Methods: A retrospective review of consecutive pediatric patients who underwent hemispheric surgery for intractable epilepsy and at least 6 months of follow-up at UCLA between 1994 and 2018 was performed. Patients were grouped by MLBS severity, shunt placement, valve type, and valve opening pressure (VOP). MLBS was evaluated using the paired samples t-test and analysis of covariance adjusting for follow-up time and baseline postoperative MLBS.
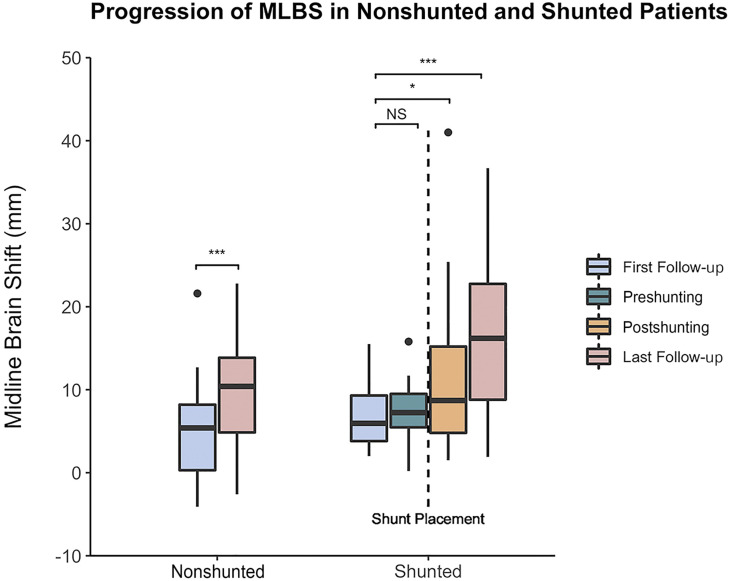
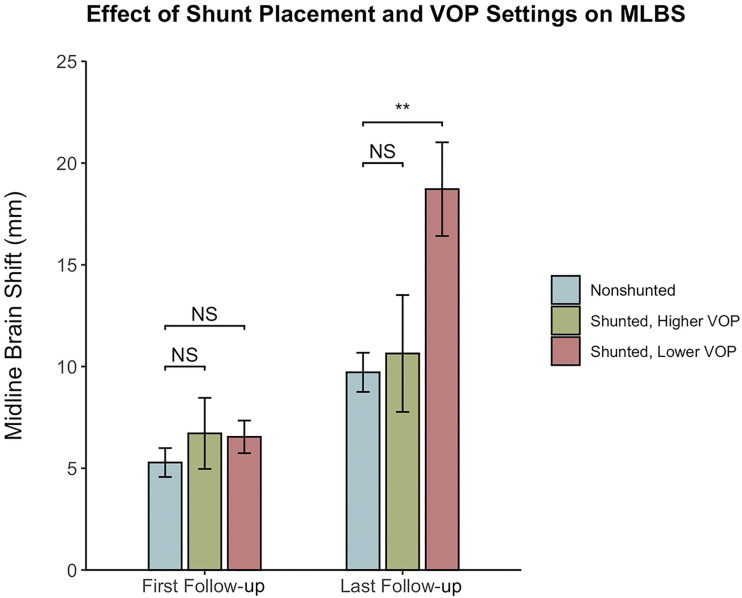
Results: Seventy patients were analyzed, of which 23 (33%) required CSF shunt placement in the ipsilateral surgical cavity for posthemispherectomy hydrocephalus. MLBS increased between first and last follow-up for nonshunted (5.3 ± 4.9-9.7 ± 6.6 mm, P < .001) and shunted (6.6 ± 3.5-16.3 ± 9.4 mm, P < .001) patients. MLBS progression was greater in shunted patients (P = .001). Shunts with higher VOPs did not increase MLBS relative to nonshunted patients (P = .834), whereas MLBS increased with lower VOPs (P = .001). Severe MLBS was associated with debilitating headaches (P = .048).
Conclusion: Patients undergoing hemispheric surgery often develop postoperative MLBS, ie, exacerbated by CSF shunting of the ipsilateral surgical cavity, specifically when using lower VOP settings. MLBS exacerbation may be related to overshunting. Severe MLBS is associated with debilitating headaches.
Copyright © Congress of Neurological Surgeons 2022. All rights reserved.
Figures
Comment in
-
Commentary: Midline Brain Shift After Hemispheric Surgery: Natural History, Clinical Significance, and Association With Cerebrospinal Fluid Diversion.Oper Neurosurg. 2022 Sep 1;23(3):e191-e192. doi: 10.1227/ons.0000000000000327. Epub 2022 Jul 11. Oper Neurosurg. 2022. PMID: 35972111 No abstract available.
References
-
- Bahuleyan B, Robinson S, Nair AR, Sivanandapanicker JL, Cohen AR. Anatomic hemispherectomy: historical perspective. World Neurosurg. 2013;80(3-4):396-398. - PubMed
-
- Beier AD, Rutka JT. Hemispherectomy: historical review and recent technical advances. Neurosurg Focus. 2013;34(6):E11. - PubMed
-
- Peacock WJ. Hemispherectomy for the treatment of intractable seizures in childhood. Neurosurg Clin N Am. 1995;6(3):549-563. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
