

Acromioclavicular joint suture button repair leads to coracoclavicular tunnel widening
- PMID: 35316368
- PMCID: PMC9859898
- DOI: 10.1007/s00167-022-06929-0
Acromioclavicular joint suture button repair leads to coracoclavicular tunnel widening
Abstract
Purpose: Biomechanical evaluation of three different suture button devices used in acromioclavicular joint repair and analysis of their effect on post-testing tunnel widening.
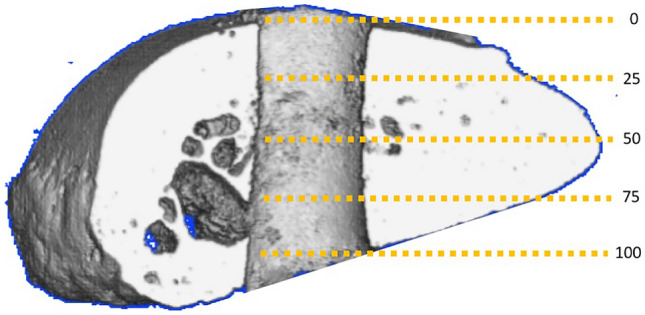
Methods: Eighteen human shoulder girdles were assigned into three groups with a similar mean bone mineral density. Three different single-tunnel acromioclavicular repair devices were tested: (1) AC TightRope® with FiberWire; (2) AC Dog Bone™ Button with FiberTape; (3) Low Profile AC Repair System. Biomechanical testing was performed simulating the complex movement of the distal clavicle as follows. A vertical load of 80 N was applied continuously. The rotation of the clavicle about its long axis was set at 10° anterior and 30° posterior for 2500 cycles at 0.25 Hz. The horizontal translation of the clavicle was set at 6 mm medial and 6 mm lateral for 10,000 cycles at 1 Hz. The coracoclavicular distance was measured before and after testing. After testing, each sample underwent micro-CT analysis. Following 3D reconstruction, the area of the bone tunnels was measured at five defined cross sections.
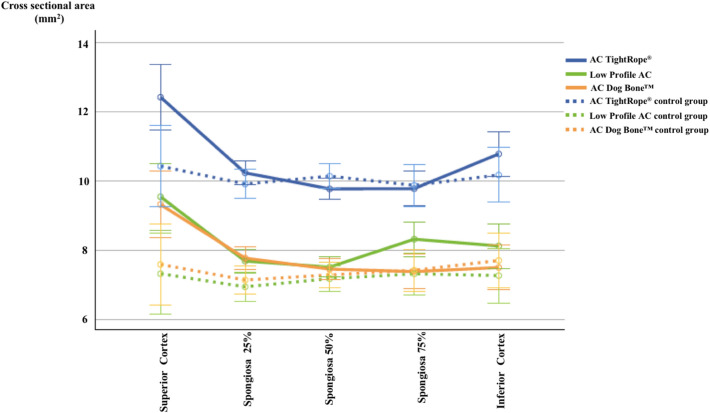
Results: In TightRope® and Dog Bone™ groups, all samples completed testing, whereas in the Low Profile group, three out of six samples showed system failure. The mean absolute difference of coracoclavicular distance after testing was significantly greater in the Low Profile group compared to TightRope® and Dog Bone™ groups (4.3 ± 1.3 mm vs 1.9 ± 0.7 mm vs 1.9 ± 0.8 mm; p = 0.001). Micro-CT analysis of the specimens demonstrated significant tunnel widening in the inferior clavicular and superior coracoid regions in all three groups (p < 0.05).
Conclusion: Significant tunnel widening can be observed for all devices and is primarily found in the inferior parts of the clavicle and superior parts of the coracoid. The Low Profile AC Repair System showed inferior biomechanical properties compared to the AC TightRope® and AC Dog Bone™ devices. Therefore, clinicians should carefully select the type of acromioclavicular repair device used and need to consider tunnel widening as a complication.
Keywords: Acromioclavicular joint; Arthroscopy; Micro-CT; Shoulder surgery; Suture button; Tunnel widening.
© 2022. The Author(s).
Conflict of interest statement
All Authors declare that they have no conflict of interest.
Figures


Similar articles
-
Evaluation of the coracoid bone tunnel placement on Dog Bone™ button fixation for acromioclavicular joint dislocation: a cadaver study combined with finite element analysis.BMC Musculoskelet Disord. 2023 Jan 9;24(1):18. doi: 10.1186/s12891-022-06119-6. BMC Musculoskelet Disord. 2023. PMID: 36624428 Free PMC article.
-
Biomechanical Evaluation of a Single- Versus Double-Tunnel Coracoclavicular Ligament Reconstruction With Acromioclavicular Stabilization for Acromioclavicular Joint Injuries.Am J Sports Med. 2018 Apr;46(5):1070-1076. doi: 10.1177/0363546517752673. Epub 2018 Feb 13. Am J Sports Med. 2018. PMID: 29438625
-
Anterior and coracoid base tunnel location combined with single -or double clavicular tunnel techniques using double-button fixation for coracoclavicular ligament reconstruction both restore horizontal stability. A biomechanical cadaver study.Clin Biomech (Bristol). 2024 Dec;120:106363. doi: 10.1016/j.clinbiomech.2024.106363. Epub 2024 Oct 12. Clin Biomech (Bristol). 2024. PMID: 39418675
-
Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques.Am J Sports Med. 2019 Sep;47(11):2745-2758. doi: 10.1177/0363546518795147. Epub 2018 Oct 1. Am J Sports Med. 2019. PMID: 30272997
-
Factors influencing clavicular tunnel widening after single bundle coracoclavicular ligament reconstruction.J Orthop Surg Res. 2024 Nov 7;19(1):735. doi: 10.1186/s13018-024-05201-0. J Orthop Surg Res. 2024. PMID: 39506765 Free PMC article. Review.
Cited by
-
No correlation exists between coracoid tunnel widening and loss of reduction after arthroscopic acromioclavicular fixation using tightrope system.Knee Surg Sports Traumatol Arthrosc. 2023 Jul;31(7):2646-2653. doi: 10.1007/s00167-023-07329-8. Epub 2023 Feb 20. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36805298 Free PMC article.
-
Evaluation of the coracoid bone tunnel placement on Dog Bone™ button fixation for acromioclavicular joint dislocation: a cadaver study combined with finite element analysis.BMC Musculoskelet Disord. 2023 Jan 9;24(1):18. doi: 10.1186/s12891-022-06119-6. BMC Musculoskelet Disord. 2023. PMID: 36624428 Free PMC article.
-
Progressive Loss of Acromioclavicular Joint Reduction Correlated with Progressive Clavicular Tunnel Widening after Coracoclavicular Stabilization in Acute High-Grade Acromioclavicular Joint Injury.J Clin Med. 2024 Jul 29;13(15):4446. doi: 10.3390/jcm13154446. J Clin Med. 2024. PMID: 39124713 Free PMC article.
-
Arthroscopically Assisted Acromioclavicular Joint Reconstruction With 2.0-mm Tunnel in the Clavicle and Suture Looping Around the Coracoid Process.Arthrosc Tech. 2025 Jan 2;14(5):103407. doi: 10.1016/j.eats.2024.103407. eCollection 2025 May. Arthrosc Tech. 2025. PMID: 40547998 Free PMC article.
-
Tendon graft through the coracoid tunnel versus under the coracoid for coracoclavicular/acromioclavicular reconstruction shows no difference in radiographic or patient-reported outcomes.Arch Orthop Trauma Surg. 2024 Aug;144(8):3491-3501. doi: 10.1007/s00402-024-05461-9. Epub 2024 Jul 18. Arch Orthop Trauma Surg. 2024. PMID: 39025979 Free PMC article. Clinical Trial.
References
-
- Berthold DP, Muench LN, Dyrna F, Uyeki CL, Cote MP, Imhoff AB, Beitzel K, Mazzocca AD. Radiographic alterations in clavicular bone tunnel width following anatomic coracoclavicular ligament reconstruction (ACCR) for chronic acromioclavicular joint injuries. Knee Surg Sports Traumatol Arthrosc. 2020;29(7):2046–2054. doi: 10.1007/s00167-020-05980-z. - DOI - PubMed
-
- Dittrich M, Wirth B, Freislederer F, Bellmann F, Scheibel M. Arthroscopically assisted stabilization of chronic bidirectional acromioclavicular joint instability using a low-profile implant and a free tendon graft: a technical note. Obere Extrem. 2020;15(2):118–121. doi: 10.1007/s11678-020-00576-y. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
