

Construction and Verification of Risk Predicting Models to Evaluate the Possibility of Venous Thromboembolism After Robot-Assisted Radical Prostatectomy
- PMID: 35316433
- PMCID: PMC9246795
- DOI: 10.1245/s10434-022-11574-5
Construction and Verification of Risk Predicting Models to Evaluate the Possibility of Venous Thromboembolism After Robot-Assisted Radical Prostatectomy
Abstract
Background: Venous thromboembolism (VTE) is the second leading cause for death of radical prostatectomy. We aimed to establish new nomogram to predict the VTE risk after robot-assisted radical prostatectomy (RARP).
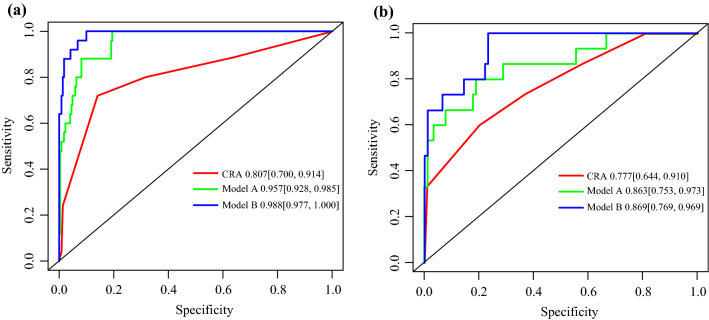
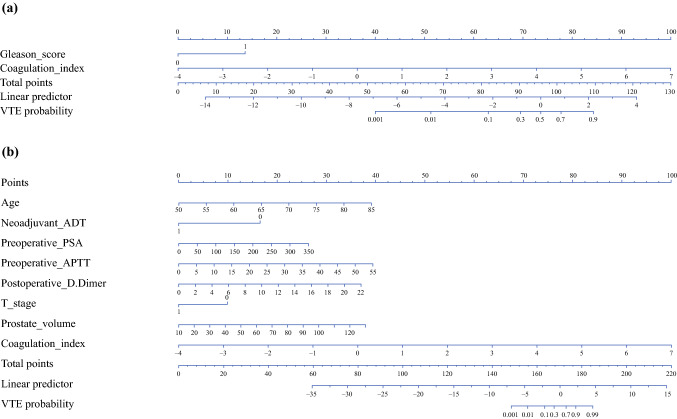
Methods: Patients receiving RARP in our center from November 2015 to June 2021, were enrolled in study. They were randomly divided into training and testing cohorts by 8:2. Univariate and multivariate logistic regression (model A) and stepwise logistic regression (model B) were used to fit two models. The net reclassification improvement (NRI), integrated discrimination improvement (IDI), and receiver operating characteristic (ROC) curve were used to compare predictive abilities of two new models with widely used Caprini risk assessment (CRA) model. Then, two nomograms were constructed and received internal validation.
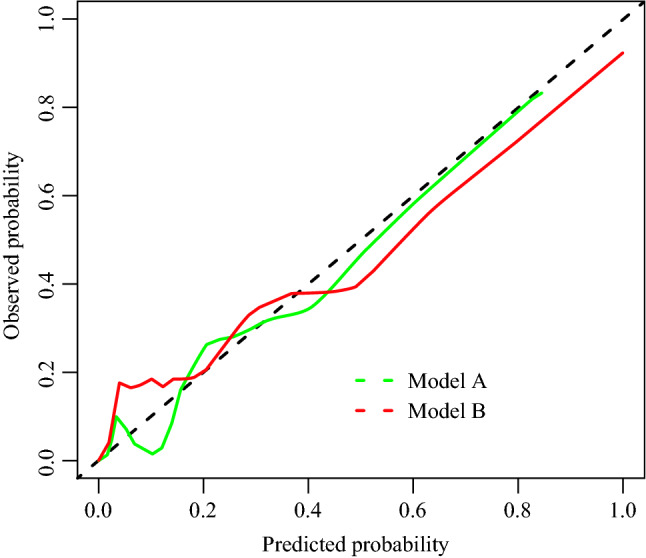
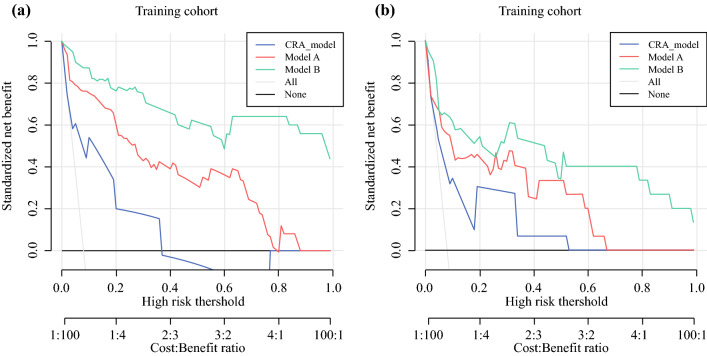
Results: Totally, 351 patients were included. The area under ROC of model A and model B were 0.967 (95% confidence interval: 0.945-0.990) and 0.978 (95% confidence interval: 0.960-0.996), which also were assayed in the testing cohorts. Both the prediction and classification abilities of the two new models were superior to CRA model (NRI > 0, IDI > 0, p < 0.05). The C-index of Model A and Model B were 0.968 and 0.978, respectively. For clinical usefulness, the two new models offered a net benefit with threshold probability between 0.08 and 1 in decision curve analysis, suggesting the two new models predict VTE events more accurately.
Conclusions: Both two new models have good prediction accuracy and are superior to CRA model. Model A has an advantage of less variable. This easy-to-use model enables rapid clinical decision-making and early intervention in high-risk groups, which ultimately benefit patients.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Developing and validating risk predicting models to assess venous thromboembolism risk after radical cystectomy.Transl Androl Urol. 2024 Sep 30;13(9):1823-1834. doi: 10.21037/tau-24-194. Epub 2024 Sep 26. Transl Androl Urol. 2024. PMID: 39434743 Free PMC article.
-
Construction and verification of risk predicting models to evaluate the possibility of hydrocephalus following aneurysmal subarachnoid hemorrhage.J Stroke Cerebrovasc Dis. 2024 Feb;33(2):107535. doi: 10.1016/j.jstrokecerebrovasdis.2023.107535. Epub 2023 Dec 21. J Stroke Cerebrovasc Dis. 2024. PMID: 38134551
-
Development and validation of a nomogram to assess postoperative venous thromboembolism risk in patients with stage IA non-small cell lung cancer.Cancer Med. 2023 Jan;12(2):1217-1227. doi: 10.1002/cam4.4982. Epub 2022 Jun 27. Cancer Med. 2023. PMID: 35758614 Free PMC article. Clinical Trial.
-
[Methods for training of robot-assisted radical prostatectomy].Khirurgiia (Mosk). 2019;(1):89-94. doi: 10.17116/hirurgia201901189. Khirurgiia (Mosk). 2019. PMID: 30789615 Review. Russian.
-
[Transperitoneal versus extraperitoneal robot-assisted radical prostatectomy for localized prostate cancer].Zhonghua Nan Ke Xue. 2017 Jun;23(6):540-549. Zhonghua Nan Ke Xue. 2017. PMID: 29722948 Review. Chinese.
Cited by
-
Developing and validating risk predicting models to assess venous thromboembolism risk after radical cystectomy.Transl Androl Urol. 2024 Sep 30;13(9):1823-1834. doi: 10.21037/tau-24-194. Epub 2024 Sep 26. Transl Androl Urol. 2024. PMID: 39434743 Free PMC article.
-
Nomogram to Assess the Risk of Deep Venous Thrombosis After Posterior Lumbar Fusion: A Retrospective Study.Global Spine J. 2025 May;15(4):2169-2175. doi: 10.1177/21925682241289119. Epub 2024 Oct 11. Global Spine J. 2025. PMID: 39390902 Free PMC article.
-
Machine learning predicts cancer-associated venous thromboembolism using clinically available variables in gastric cancer patients.Heliyon. 2023 Jan 3;9(1):e12681. doi: 10.1016/j.heliyon.2022.e12681. eCollection 2023 Jan. Heliyon. 2023. PMID: 36632097 Free PMC article.
-
Predictive accuracy of boosted regression model in estimating risk of venous thromboembolism following minimally invasive radical surgery in pharmacological prophylaxis-naïve men with prostate cancer.World J Surg Oncol. 2024 Feb 23;22(1):67. doi: 10.1186/s12957-023-03170-y. World J Surg Oncol. 2024. PMID: 38395873 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
