

The Association Between Sustained HbA1c Control and Long-Term Complications Among Individuals with Type 2 Diabetes: A Retrospective Study
- PMID: 35316502
- PMCID: PMC9056490
- DOI: 10.1007/s12325-022-02106-4
The Association Between Sustained HbA1c Control and Long-Term Complications Among Individuals with Type 2 Diabetes: A Retrospective Study
Abstract
Introduction: The prevalence of type 2 diabetes (T2D) represents a rising burden in the US and worldwide, with the condition shown to be associated with relatively large human and economic costs. Part of the reason for such high costs associated with T2D is that the condition is often accompanied by additional health-related complications. The goal of this research is to examine the association between glycemic control and diabetes-related complications for individuals with T2D.
Methods: The Optum Clinformatics® Data Mart (CDM) database from 2007 to 2020 was used to identify adults with T2D. Individuals were classified as having sustained glycemic control (all hemoglobin A1c [HbA1c] < 7%) or poor glycemic control (all HbA1c ≥ 7%) over the 5-year post-period, and diabetes-related complications were identified based upon the Diabetes Complications Severity Index. Multivariable analyses examined the association between sustained glycemic control and diagnosis of a diabetes-related complication in the post-period.
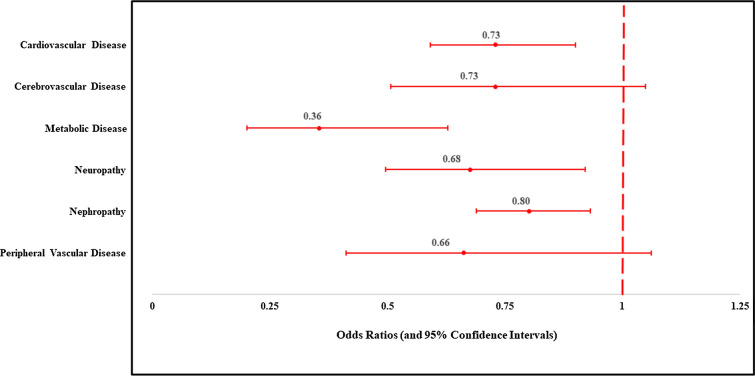
Results: Maintaining HbA1c < 7% over the 5-year post-period, compared to maintaining HbA1c ≥ 7%, was associated with reduced odds of the diabetes-related complications of cardiovascular disease (odds ratio [OR] = 0.76, 95% confidence interval [CI] 0.61-0.94), metabolic disease (OR = 0.37, 95% CI 0.22-0.600), neuropathy (OR = 0.62, 95% CI 0.45-0.84), nephropathy (OR = 0.81, 95% CI 0.69-0.94), and peripheral vascular disease (OR = 0.52, 95% CI 0.33-0.83). There was no statistically significant association between sustained glycemic control and cerebrovascular disease.
Conclusions: Sustained glycemic control was found to be associated with significant reductions in the odds of being diagnosed with diabetes-related complications over a 5-year post-period.
Keywords: Complications; Diabetes complications severity index; Hemoglobin A1c (HbA1c); Odds ratios (OR); Type 2 diabetes (T2D).
© 2022. The Author(s).
Figures



Similar articles
-
Metabolic memory: Evolving concepts.J Diabetes. 2018 Mar;10(3):186-187. doi: 10.1111/1753-0407.12622. Epub 2017 Dec 11. J Diabetes. 2018. PMID: 29091343
-
Effect of glycemic control on the Diabetes Complications Severity Index score and development of complications in people with newly diagnosed type 2 diabetes.J Diabetes. 2018 Mar;10(3):192-199. doi: 10.1111/1753-0407.12613. Epub 2017 Nov 27. J Diabetes. 2018. PMID: 28976724
-
Divergent impacts of glycemic control on mortality and complications in patients with early-versus late-onset type 2 diabetes: A retrospective cohort study.PLoS One. 2025 May 23;20(5):e0322886. doi: 10.1371/journal.pone.0322886. eCollection 2025. PLoS One. 2025. PMID: 40408408 Free PMC article.
-
[Indicators of glycemic control --hemoglobin A1c (HbA1c), glycated albumin (GA), and 1,5-anhydroglucitol (1,5-AG)].Rinsho Byori. 2014 Jan;62(1):45-52. Rinsho Byori. 2014. PMID: 24724426 Review. Japanese.
-
Rapid-Acting Insulin Analogues Versus Regular Human Insulin: A Meta-Analysis of Effects on Glycemic Control in Patients with Diabetes.Diabetes Ther. 2020 Mar;11(3):573-584. doi: 10.1007/s13300-019-00732-w. Epub 2019 Dec 23. Diabetes Ther. 2020. PMID: 31873857 Free PMC article. Review.
Cited by
-
Cost-effectiveness of Semaglutide Compared With Other Glucose-Lowering Medications in Treating Type 2 Diabetes: A Comprehensive Systematic Review and Meta-analysis.Diabetes Care. 2025 Jun 1;48(6):1032-1041. doi: 10.2337/dc24-2241. Diabetes Care. 2025. PMID: 40392993 Free PMC article. Review.
-
The Impact of Home Care on Glycosylated Hemoglobin and Quality of Life in Type 2 Diabetes Patients Discharged After Surgery.SAGE Open Nurs. 2025 Aug 14;11:23779608251365336. doi: 10.1177/23779608251365336. eCollection 2025 Jan-Dec. SAGE Open Nurs. 2025. PMID: 40821011 Free PMC article.
-
Sustained weight reduction following 12 weeks of intermittent fasting intervention in people with insulin-treated type 2 diabetes-Two-year follow-up of the randomised controlled InterFast-2 trial.Diabetes Obes Metab. 2025 Mar;27(3):1605-1608. doi: 10.1111/dom.16158. Epub 2025 Jan 2. Diabetes Obes Metab. 2025. PMID: 39748228 Free PMC article. No abstract available.
-
Laughter yoga as an enjoyable therapeutic approach for glycemic control in individuals with type 2 diabetes: A randomized controlled trial.Front Endocrinol (Lausanne). 2023 Mar 31;14:1148468. doi: 10.3389/fendo.2023.1148468. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37065750 Free PMC article. Clinical Trial.
-
Association between dietary mineral intake and new onset diabetes/pre-diabetes after chronic pancreatitis.Front Nutr. 2025 Jan 7;11:1461468. doi: 10.3389/fnut.2024.1461468. eCollection 2024. Front Nutr. 2025. PMID: 39839287 Free PMC article.
References
-
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020 [Internet]. Washington DC: U.S. Department of Health & Human Services; [Updated 2020 February 11; Cited 2021 December 12]. https://www.cdc.gov/diabetes/library/features/diabetes-stat-report.html.
-
- Alzaid A, Ladrón de Guevara P, Beillat M, Lehner MV, Atanasov P. Burden of disease and costs associated with type 2 diabetes in emerging and established markets: systematic review analyses. Expert Rev Pharmacoecon Outcomes Res. 2021;21(4):785–798. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
