

Fibrinolytic assays in bleeding of unknown cause: Improvement in diagnostic yield
- PMID: 35316940
- PMCID: PMC8922970
- DOI: 10.1002/rth2.12681
Fibrinolytic assays in bleeding of unknown cause: Improvement in diagnostic yield
Abstract
Introduction: Analysis of fibrinolytic disorders is challenging and may potentially lead to underdiagnosis of patients with an increased bleeding tendency.
Aim: To compare clinical characteristics, laboratory measurements, and treatment modalities in a monocenter cohort of patients in whom fibrinolytic studies were performed.
Methods: Retrospective study of patients in whom fibrinolytic studies were performed between January 2016 and February 2020 in the Hemophilia Treatment Center, Nijmegen-Eindhoven-Maastricht, the Netherlands. Plasminogen activator inhibitor type 1 (PAI-1) antigen and activity level, α2-antiplasmin activity, tissue plasminogen activator, and euglobulin clot lysis time (ECLT) before and after venous compression were determined in all patients. Data of bleeding assessment tool (BAT) score, clinical characteristics, results of primary and secondary hemostasis assays, and general treatment plans were collected.
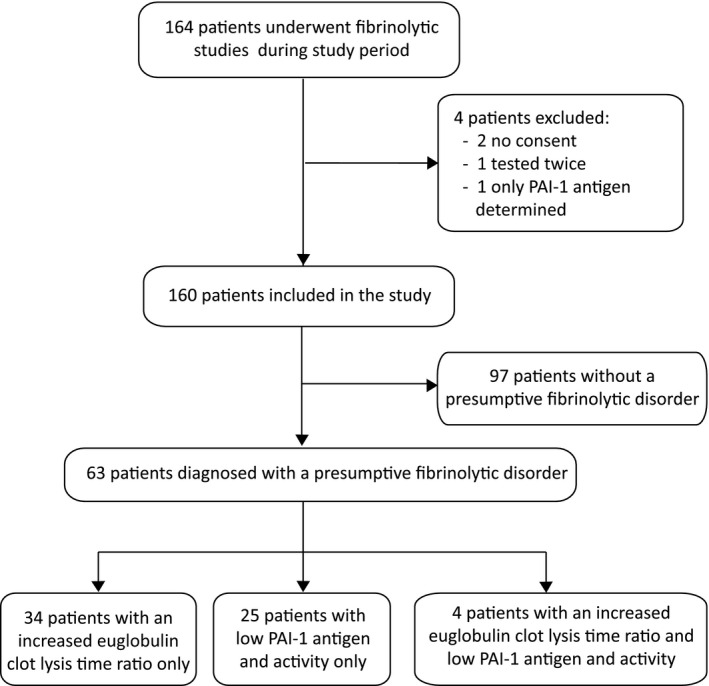
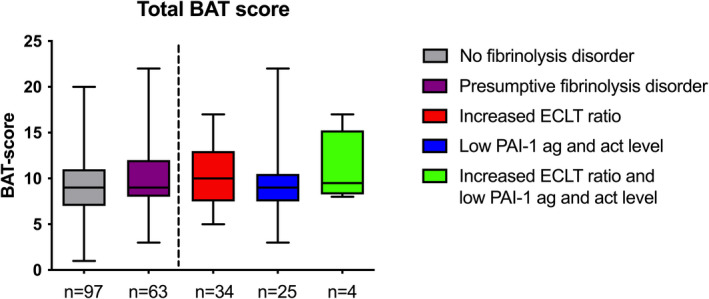
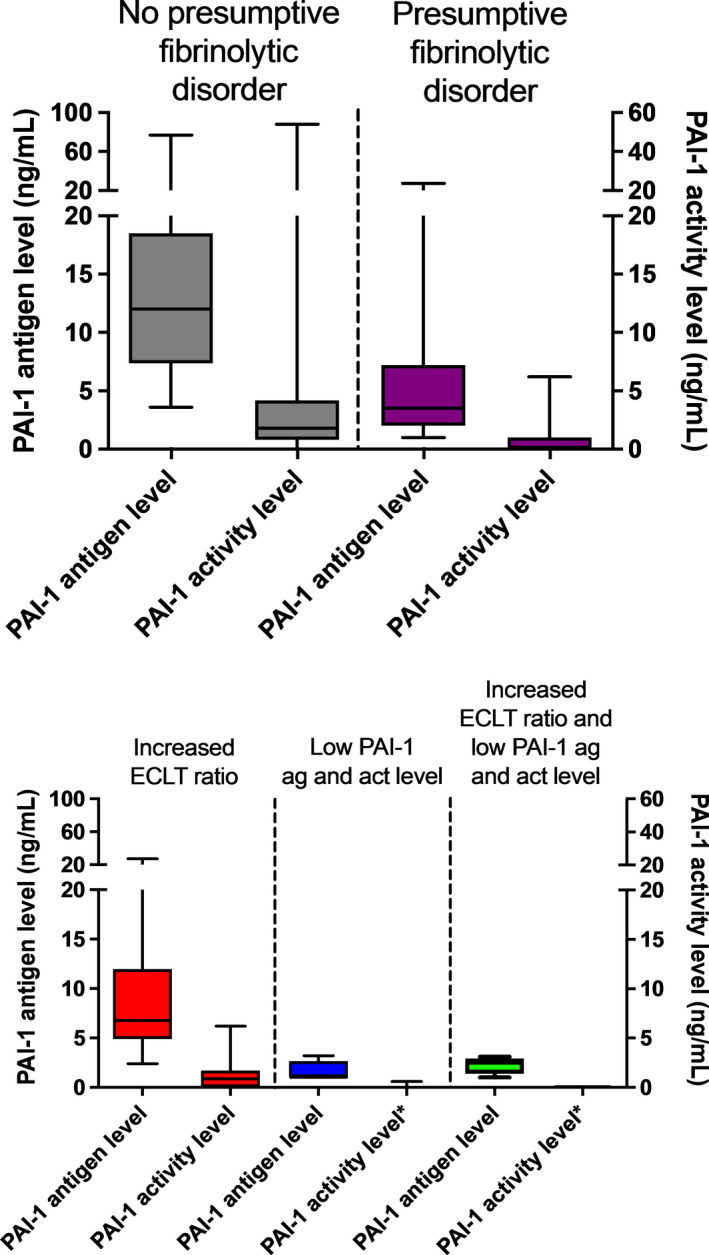
Results: In total, 160 patients were included: 97 (61%) without and 63 (39%) with a laboratory-based fibrinolytic disorder. Mean BAT score did not differ between the groups (9.3 vs 9.8, respectively). The presumptive fibrinolytic disorders were distributed as follows: 34 patients had an increased ECLT ratio or low baseline ECLT, 25 patients had low PAI-1 antigen and activity level, and four patients had both. The majority of these patients were treated with tranexamic acid monotherapy (60%) with only 40% additional treatment options, whereas 80% of patients without a presumptive fibrinolytic disorder had multiple treatment modalities.
Discussion: Analysis of fibrinolytic disorders in selected patients has a high diagnostic yield. General incorporation of fibrinolytic analysis in the diagnostic workup of patients with bleeding of unknown cause can improve diagnosis and management of their bleeding episodes.
Keywords: bleeding of unknown cause; fibrin clot lysis time; fibrinolysis; plasminogen activator inhibitor 1; tissue plasminogen activator; tranexamic acid.
© 2022 The Authors. Research and Practice in Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis (ISTH).
Figures

Similar articles
-
Systematic elucidation of effects of tranexamic acid on fibrinolysis and bleeding during and after cardiopulmonary bypass surgery.Thromb Res. 2001 Dec 1;104(5):301-7. doi: 10.1016/s0049-3848(01)00379-6. Thromb Res. 2001. PMID: 11738071 Clinical Trial.
-
Development and application of global assays of hyper- and hypofibrinolysis.Res Pract Thromb Haemost. 2019 Nov 6;4(1):46-53. doi: 10.1002/rth2.12275. eCollection 2020 Jan. Res Pract Thromb Haemost. 2019. PMID: 31989084 Free PMC article.
-
Laboratory evaluation of a new integrative assay to phenotype plasma fibrinolytic system.Thromb J. 2022 Dec 5;20(1):73. doi: 10.1186/s12959-022-00435-6. Thromb J. 2022. PMID: 36471371 Free PMC article.
-
Inherited disorders of the fibrinolytic pathway.Transfus Apher Sci. 2019 Oct;58(5):572-577. doi: 10.1016/j.transci.2019.08.007. Epub 2019 Aug 8. Transfus Apher Sci. 2019. PMID: 31427261 Review.
-
Recognition of Plasminogen Activator Inhibitor Type 1 as the Primary Regulator of Fibrinolysis.Curr Drug Targets. 2019;20(16):1695-1701. doi: 10.2174/1389450120666190715102510. Curr Drug Targets. 2019. PMID: 31309890 Free PMC article. Review.
Cited by
-
Plasmin generation analysis in patients with bleeding disorder of unknown cause.Blood Adv. 2024 Nov 12;8(21):5663-5673. doi: 10.1182/bloodadvances.2024012855. Blood Adv. 2024. PMID: 39231312 Free PMC article.
-
Targeted exome analysis in patients with rare bleeding disorders: data from the Rare Bleeding Disorders in the Netherlands study.Res Pract Thromb Haemost. 2024 Jun 17;8(4):102477. doi: 10.1016/j.rpth.2024.102477. eCollection 2024 May. Res Pract Thromb Haemost. 2024. PMID: 39076726 Free PMC article.
-
Current Practice Regarding Bleeding Disorders of Unknown Cause in the Netherlands: A National Survey.Haemophilia. 2025 Jul;31(4):752-760. doi: 10.1111/hae.70065. Epub 2025 May 27. Haemophilia. 2025. PMID: 40421900 Free PMC article.
-
Bleeding disorder of unknown cause: an illustrated review on current practice, knowledge gaps, and future perspectives.Res Pract Thromb Haemost. 2024 Nov 13;8(8):102625. doi: 10.1016/j.rpth.2024.102625. eCollection 2024 Nov. Res Pract Thromb Haemost. 2024. PMID: 39687924 Free PMC article.
-
Enhanced thrombin and plasmin generation profiles in alpha-2-antiplasmin-deficient patients: Data from the Rare Bleeding disorders in the Netherlands study.Res Pract Thromb Haemost. 2024 Oct 23;8(7):102604. doi: 10.1016/j.rpth.2024.102604. eCollection 2024 Oct. Res Pract Thromb Haemost. 2024. PMID: 39628652 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
