

Cavernous hemangioma of an intrapancreatic accessory spleen mimicking a pancreatic tumor: A case report
- PMID: 35317146
- PMCID: PMC8891771
- DOI: 10.12998/wjcc.v10.i6.1973
Cavernous hemangioma of an intrapancreatic accessory spleen mimicking a pancreatic tumor: A case report
Abstract
Background: Intrapancreatic accessory spleen (IPAS) is an uncommon condition, with the majority of cases presenting as solid lesions. Thus, this condition is frequently misdiagnosed as pancreatic solid neoplasm. Moreover, splenic cavernous hemangioma is a rare disorder, whereas lesions with a cystic appearance arising from IPAS have not been reported.
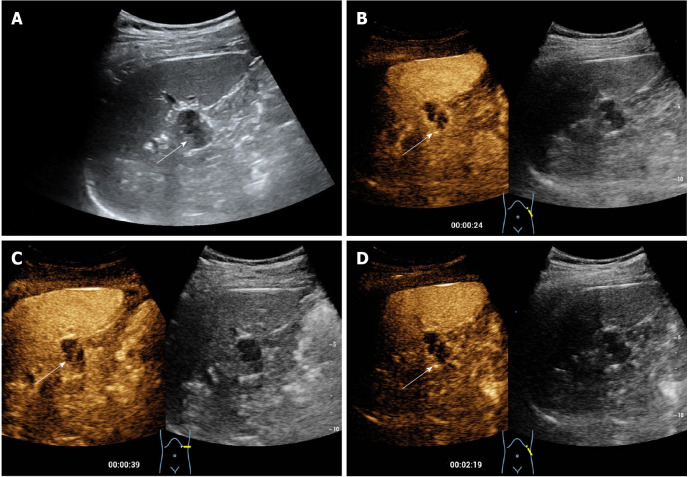
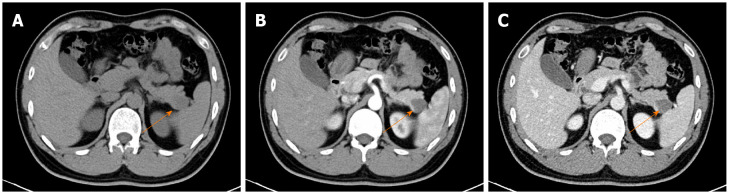
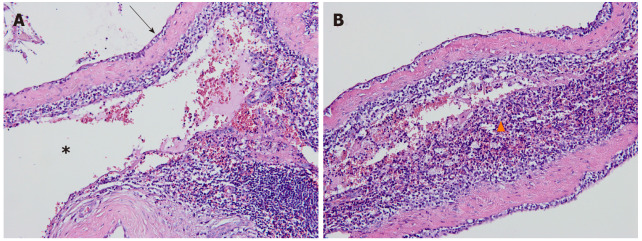
Case summary: Herein, we present a case involving a 32-year-old male who had a complex cystic lesion in the tail of the pancreas revealed by conventional ultrasound. The lesion was misdiagnosed as a pancreatic cystadenoma because of its confusing anatomic location, as well as due to its peripheral nodular and internal septal enhancement patterns on contrast-enhanced ultrasound. After multidisciplinary discussion, the patient finally underwent laparoscopic pancreatic body and tail resections. Postoperative pathology demonstrated the lesion to be a cavernous hemangioma arising from the IPAS.
Conclusion: Cavernous hemangioma in the intrapancreatic accessory spleen may mimic pancreatic cystadenoma, which is a condition with the potential to be malignant. Imaging follow-ups or surgical interventions may be helpful for the exclusion of malignant risks in complicated cystic lesions, especially those with parietal and septal enhancements.
Keywords: Case report; Contrast enhanced ultrasound; Diagnosis; Intrapancreatic accessary spleen; Pancreas.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Post-splenectomy intrapancreatic accessory spleen mimicking endocrine tumor of the pancreas.Int J Surg Case Rep. 2014;5(12):1151-3. doi: 10.1016/j.ijscr.2014.11.032. Epub 2014 Nov 15. Int J Surg Case Rep. 2014. PMID: 25437661 Free PMC article.
-
A Case of İntrapancreatic Accessory Spleen Mimicking a Pancreatic Metastasis on the 18 F-FDG PET/CT Scan: A Case with Breast Cancer.Indian J Radiol Imaging. 2021 Dec 13;31(4):1062-1064. doi: 10.1055/s-0041-1739384. eCollection 2021 Oct. Indian J Radiol Imaging. 2021. PMID: 35136530 Free PMC article.
-
Significance of imaging findings in the diagnosis of heterotopic spleen-an intrapancreatic accessory spleen (IPAS): Case report.Medicine (Baltimore). 2017 Dec;96(52):e9040. doi: 10.1097/MD.0000000000009040. Medicine (Baltimore). 2017. PMID: 29384897 Free PMC article.
-
Intrapancreatic accessory spleen: CT appearance and differential diagnosis.Abdom Imaging. 2012 Oct;37(5):812-27. doi: 10.1007/s00261-011-9830-x. Abdom Imaging. 2012. PMID: 22160284 Review.
-
Intrapancreatic accessory spleen (IPAS): A single-institution experience and review of the literature.Am J Surg. 2017 Apr;213(4):816-820. doi: 10.1016/j.amjsurg.2016.11.030. Epub 2016 Nov 23. Am J Surg. 2017. PMID: 27894508 Review.
Cited by
-
Misdiagnosis of pancreatic intraductal papillary mucinous neoplasms and the challenge of mimicking lesions: imaging diagnosis and differentiation strategies.Abdom Radiol (NY). 2025 May;50(5):2241-2257. doi: 10.1007/s00261-024-04551-x. Epub 2024 Sep 27. Abdom Radiol (NY). 2025. PMID: 39327307 Review.
-
Solid and cystic intrapancreatic accessory spleen: report of 10 cases in a single institution.Ann Med. 2025 Dec;57(1):2463564. doi: 10.1080/07853890.2025.2463564. Epub 2025 Feb 10. Ann Med. 2025. PMID: 39927469 Free PMC article.
-
Pancreatic cavernous hemangioma complicated with chronic intracapsular spontaneous hemorrhage: A case report and review of literature.World J Clin Cases. 2023 Aug 16;11(23):5615-5621. doi: 10.12998/wjcc.v11.i23.5615. World J Clin Cases. 2023. PMID: 37637682 Free PMC article.
-
Case Report: A rare case of hemorrhagic cystic IPAS masquerading as pancreatic neoplasm.Front Oncol. 2025 Jul 11;15:1626836. doi: 10.3389/fonc.2025.1626836. eCollection 2025. Front Oncol. 2025. PMID: 40718828 Free PMC article.
References
-
- Li BQ, Xu XQ, Guo JC. Intrapancreatic accessory spleen: a diagnostic dilemma. HPB (Oxford) 2018;20:1004–1011. - PubMed
-
- Halpert B, Gyorkey F. Lesions observed in accessory spleens of 311 patients. Am J Clin Pathol. 1959;32:165–168. - PubMed
-
- Sica GT, Reed MF. Case 27: intrapancreatic accessory spleen. Radiology. 2000;217:134–137. - PubMed
-
- Jang KM, Kim SH, Lee SJ, Park MJ, Lee MH, Choi D. Differentiation of an intrapancreatic accessory spleen from a small (<3-cm) solid pancreatic tumor: value of diffusion-weighted MR imaging. Radiology. 2013;266:159–167. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
