

Surgery and antibiotics for the treatment of lupus nephritis with cerebral abscesses: A case report
- PMID: 35317158
- PMCID: PMC8891782
- DOI: 10.12998/wjcc.v10.i6.1981
Surgery and antibiotics for the treatment of lupus nephritis with cerebral abscesses: A case report
Abstract
Background: Systemic lupus erythematosus (SLE) patients are extremely susceptible to opportunistic infections due to glucocorticoid and immunosuppressive treatments, which often occur in the respiratory system, the urinary system and the skin. However, multiple cerebral infections are rarely reported and their treatment is not standardized, especially when induced by a rare pathogen.
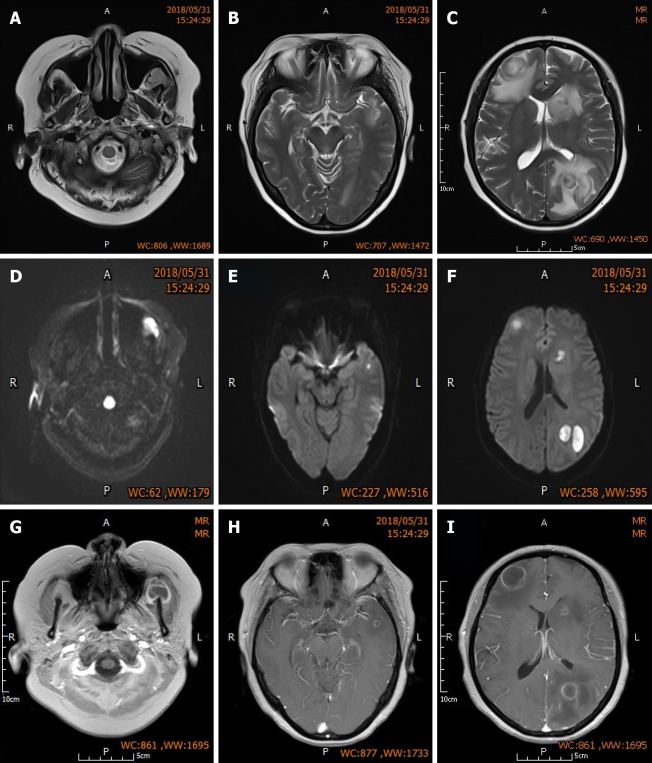
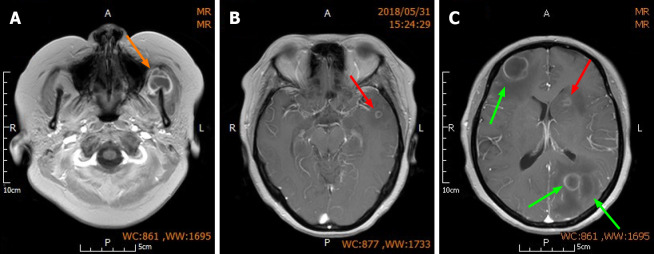
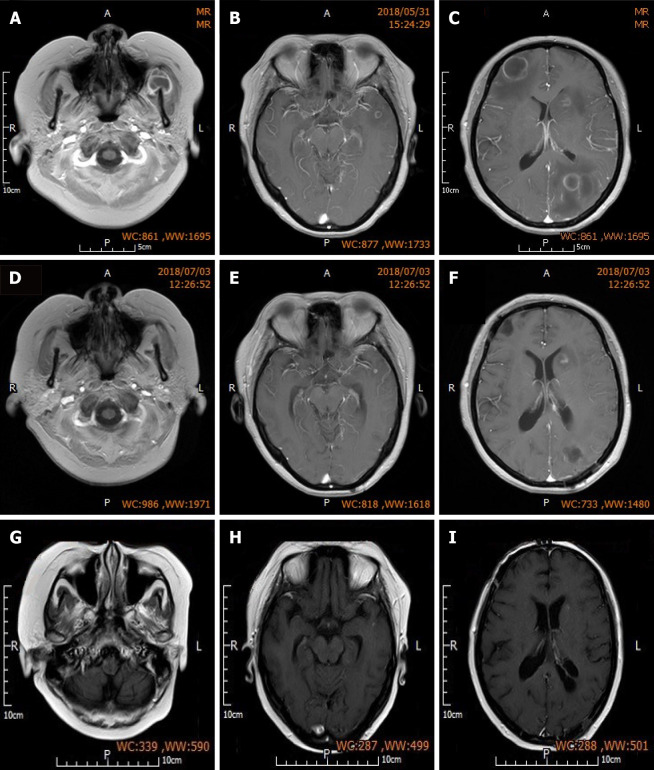
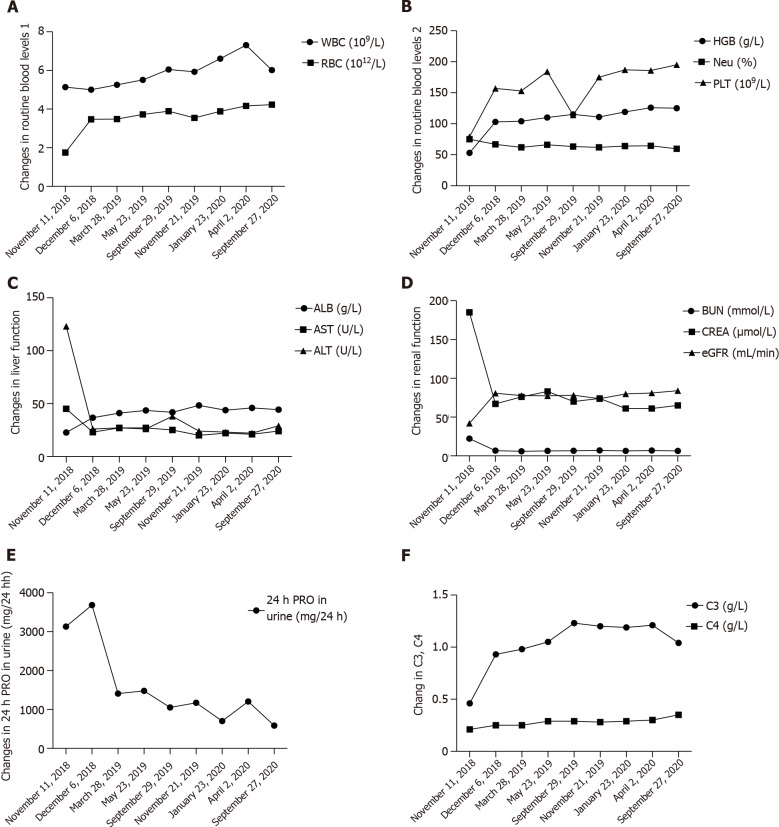
Case summary: A 46-year-old woman was treated with glucocorticoid and immunosuppressant for SLE involving the hematologic system and kidneys (class IV-G lupus nephritis) for more than one year. She was admitted to hospital due to headache and fever, and was diagnosed with multiple cerebral abscesses. Brain enhanced magnetic resonance imaging showed multiple nodular abnormal signals in both frontal lobes, left parietal and temporal lobes, left masseteric space (left temporalis and masseter region). The initial surgical plan was only to remove the large abscesses in the left parietal lobe and right frontal lobe. After surgery, based on the drug susceptibility test results (a rare pathogen Nocardia asteroides was found) and taking into consideration the patient's renal dysfunction, a multi-antibiotic regimen was selected for the treatment. The immunosuppressant mycophenolate mofetil was discontinued on admission and the dose of prednisone was reduced from 20 mg/d to 10 mg/d. Re-examination at 3 mo post-surgery showed that the intracranial lesions were reduced, the edema around the lesions was absorbed and dissipated, and her neurological symptoms had disappeared. The patient had no headaches or other neurological symptoms and lupus nephritis was stable during the 2-year follow-up period.
Conclusion: In this report, we provide reasonable indications for immunosuppression, anti-infective therapy and individualized surgery for an SLE patient complicated with multiple cerebral abscesses caused by a rare pathogen, which may help improve the diagnosis and treatment of similar cases.
Keywords: Case report; Multi-antibiotic therapy; Multiple cerebral abscesses; Nocardia asteroides; Systemic lupus erythematosus.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Rowell Syndrome in Nigeria: Systemic Lupus Erythematosus Presenting as Recurrent Erythema Multiforme in a Young Woman.Acta Dermatovenerol Croat. 2019 Sep;27(3):200-201. Acta Dermatovenerol Croat. 2019. PMID: 31542069
-
Systemic lupus erythematosus with disseminated aspergillosis misdiagnosed as lupus encephalopathy: a case report and literature review.Ann Transl Med. 2022 Oct;10(20):1147. doi: 10.21037/atm-22-4362. Ann Transl Med. 2022. PMID: 36388809 Free PMC article.
-
Uncommon Presentation of Systemic Lupus Erythematosus: Intracranial Mass Lesions as the First Manifestation.Am J Case Rep. 2024 Jun 3;25:e942877. doi: 10.12659/AJCR.942877. Am J Case Rep. 2024. PMID: 38829826 Free PMC article.
-
Primary central nervous system lymphoma in a patient with neuropsychiatric systemic lupus erythematosus receiving mycophenolate mofetil: A case report and literature review.Mod Rheumatol Case Rep. 2022 Jan 7;6(1):36-40. doi: 10.1093/mrcr/rxab012. Mod Rheumatol Case Rep. 2022. PMID: 34505624 Review.
-
Cerebral venous sinus thrombosis and subdural hematoma in a female patient with systemic lupus erythematosus: a case report and literature review.Ann Palliat Med. 2021 Jul;10(7):8454-8459. doi: 10.21037/apm-20-2285. Epub 2021 Apr 26. Ann Palliat Med. 2021. PMID: 33977732 Review.
References
-
- Keeling SO, Alabdurubalnabi Z, Avina-Zubieta A, Barr S, Bergeron L, Bernatsky S, Bourre-Tessier J, Clarke A, Baril-Dionne A, Dutz J, Ensworth S, Fifi-Mah A, Fortin PR, Gladman DD, Haaland D, Hanly JG, Hiraki LT, Hussein S, Legault K, Levy D, Lim L, Matsos M, McDonald EG, Medina-Rosas J, Pardo Pardi J, Peschken C, Pineau C, Pope J, Rader T, Reynolds J, Silverman E, Tselios K, Suitner M, Urowitz M, Touma Z, Vinet E, Santesso N. Canadian Rheumatology Association Recommendations for the Assessment and Monitoring of Systemic Lupus Erythematosus. J Rheumatol. 2018;45:1426–1439. - PubMed
-
- Vargas PJ, King G, Navarra SV. Central nervous system infections in Filipino patients with systemic lupus erythematosus. Int J Rheum Dis. 2009;12:234–238. - PubMed
-
- Horta-Baas G, Guerrero-Soto O, Barile-Fabris L. Central nervous system infection by Listeria monocytogenes in patients with systemic lupus erythematosus: analysis of 26 cases, including the report of a new case. Reumatol Clin. 2013;9:340–347. - PubMed
-
- Rudasill SE, Sanaiha Y, Xing H, Mardock AL, Khoury H, Jaman R, Ebrahimi R, Benharash P. Association of Autoimmune Connective Tissue Disease and Outcomes in Patients Undergoing Transcatheter Aortic Valve Implantation. Am J Cardiol. 2019;123:1675–1680. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
