

Plate vs reverse shoulder arthroplasty for proximal humeral fractures: The psychological health influence the choice of device?
- PMID: 35317248
- PMCID: PMC8935332
- DOI: 10.5312/wjo.v13.i3.297
Plate vs reverse shoulder arthroplasty for proximal humeral fractures: The psychological health influence the choice of device?
Abstract
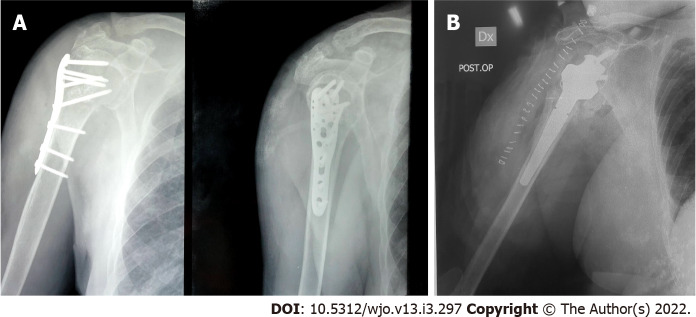
Background: Proximal humeral fractures represent the third most common observed osteoporotic fracture; the treatment in three and four-part proximal humeral fractures in patients over 65 years is still controversial. Among the treatments described in literature, open reduction and internal fixation (O.R.I.F) and reverse shoulder arthroplasty (RSA) are gaining an increasing popularity.
Aim: To investigate the correct treatment for three and four-part proximal humeral fractures according to psychological aspects.
Methods: It was conducted a prospective study with a series of 63 patients treated with O.R.I.F. (group A) and with RSA (group B) for three and four-part proximal humeral fractures according to Neer classification system. A conservative treatment group, as control, was finally introduced. One independent observer performed clinical and a psychological evaluation at one (T0), six (T1) and twelve months (T2) postoperatively. The Constant's score and The Disabilities of the Arm, Shoulder and Hand (DASH score) were used for clinical evaluation, while General Anxiety Disorder-7 (GAD-7) and Caregiver Strain Scale (CSS) were used for psychological evaluation.
Results: At one month follow up in group A the mean values were DASH score 50.8, Constant score 36.1, GAD-7 score 5.4, CSS 5.0. For the group B, the average values at T0 were: DASH score 54.6, Constant score 32.0; GAD-7 score 6.4, CSS 6.2. At six months in group A the average values were DASH score 42.1, Constant score 47.3, GAD-7 score 4.3, CSS 3.9. For the group B, the average values at T1 were: DASH score 39.1, Constant score 43.2, GAD-7 score 5.7, CSS 5.5. At twelve months in the group A, the mean values were DASH score 32.8, Constant score 60.0, GAD-7 score 3.2, CSS 3.1. For the group B shown these mean values: DASH score 33.6, Constant score 52.9, GAD-7 score 4.3, CSS 4.5. We demonstrated a better clinical and psychological outcome at T2 in the group treated with osteosynthesis compared to the group treated with arthroplasty (Constant P = 0.049, GAD-7 P = 0.012 and CSS P = 0.005). A better clinical and psychological outcome emerged in control group at T2 comparing with surgical group (DASH score P = 0.014, Constant score P < 0.001, GAD-7 P = 0.002 and CSS P = 0.001).
Conclusion: Both open osteosynthesis and reverse shoulder arthroplasty are valid treatments for proximal humeral fractures. According to the best osteosynthesis results the authors suggested to perform a psychological analysis for each patient in order to choose the appropriate treatment.
Keywords: Caregiver Strain scale; General Anxiety Disorder-7 scale; Open reduction and fixation; Proximal humerus fractures; Psychological health; Reverse shoulder arthroplasty.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that there are no conflicts of interest regarding the publication of this paper.
Figures
References
-
- Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury. 2006;37:691–697. - PubMed
-
- Lauritzen JB, Schwarz P, Lund B, McNair P, Transbøl I. Changing incidence and residual lifetime risk of common osteoporosis-related fractures. Osteoporos Int. 1993;3:127–132. - PubMed
-
- Seeley DG, Browner WS, Nevitt MC, Genant HK, Scott JC, Cummings SR. Which fractures are associated with low appendicular bone mass in elderly women? Ann Intern Med. 1991;115:837–842. - PubMed
-
- Launonen AP, Lepola V, Saranko A, Flinkkilä T, Laitinen M, Mattila VM. Epidemiology of proximal humerus fractures. Arch Osteoporos. 2015;10:209. - PubMed
-
- van Staa TP, Dennison EM, Leufkens HG, Cooper C. Epidemiology of fractures in England and Wales. Bone. 2001;29:517–522. - PubMed
LinkOut - more resources
Full Text Sources
