

Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
- PMID: 35317250
- PMCID: PMC8935330
- DOI: 10.5312/wjo.v13.i3.267
Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
Abstract
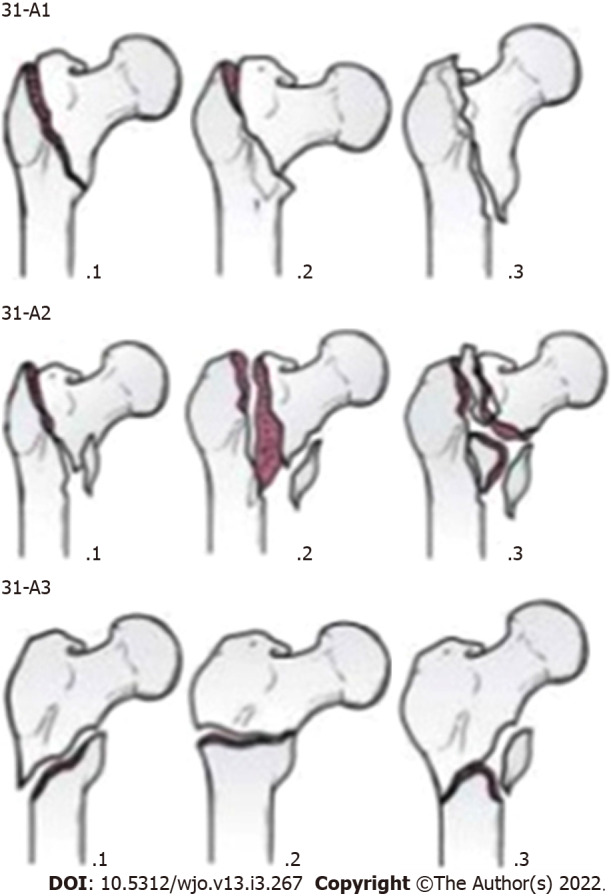
Background: Intertrochanteric (IT) fracture is one of the most common fractures seen in an orthopaedic practice. Proximal femoral nailing (PFN) is a common modality of fixing IT femur fracture. We retrospectively studied whether a PFN with two proximal lag screws can be done without distal interlocking screws in the 31-A1 and 31-A2 fracture patterns according to the Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association (AO/OTA) guidelines for IT femur fractures.
Aim: To compare the outcomes of IT fractures (AO/OTA 31-A1 and 31-A2) treated by PFN with and without distal interlocking screws.
Methods: We carried out a retrospective study of 140 patients in a tertiary care centre who had AO/OTA type 31-A1 and 31-A2 IT fractures. We divided the patients into two groups, in which one of the groups received distal interlocking screws (group 1) and the other group did not (group 2). The subjects were followed up for a mean period of 14 mo and assessed for radiological union time, fracture site collapse, mechanical stability of implant, and complications associated with the PFN with distal interlocking and without distal interlocking. Then, the results were compared.
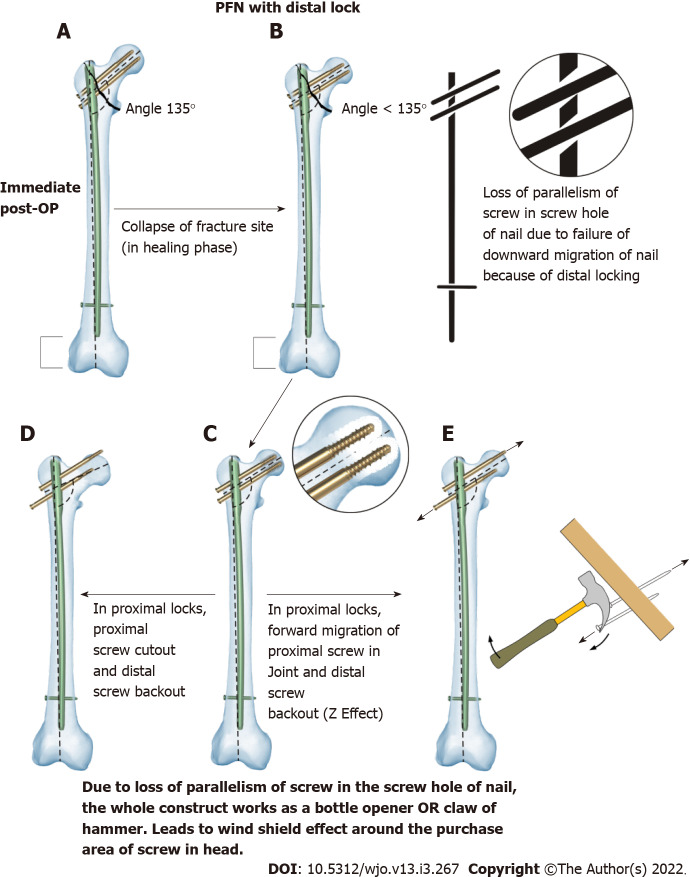
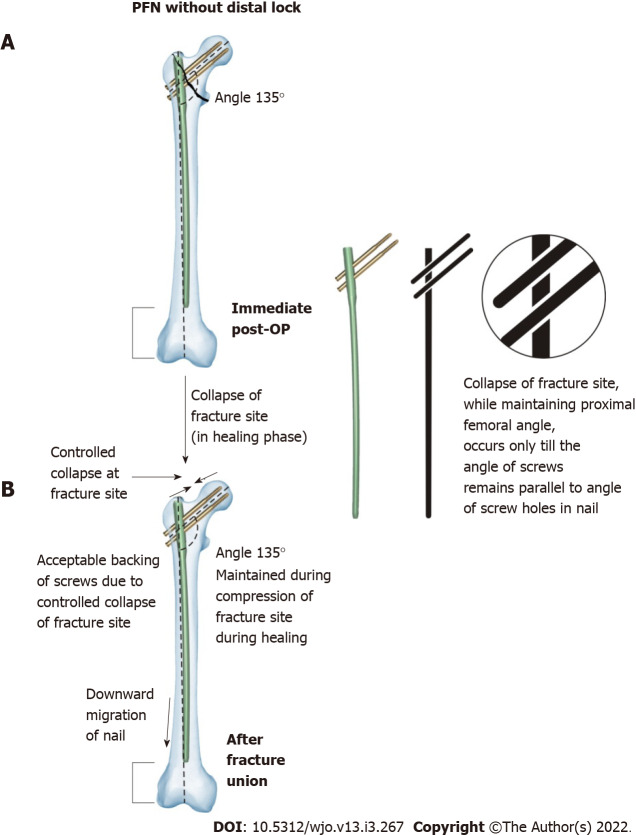
Results: PFN without distal interlocking screws has several advantages and gives better results over PFN with distal interlocking screws in the AO/OTA 31-A2 fracture pattern. However, similar results were observed in both groups with the fracture pattern AO/OTA 31-A1. In patients with fracture pattern AO/OTA 31-A2 treated by PFN without distal interlocking screws, there were minimal proximal lock-related complications and no risk of distal interlock-related complications. The operative time, IITV radiation time and time to radiological union were reduced. These patients also had better rotational alignment of the proximal femur, and the anatomy of the proximal femur was well maintained. It was also noted that in the cases where distal interlocking was performed, there was a gradual decrease in neck shaft angle, which led to varus collapse and failure of bone-implant construct in 21.40%.
Conclusion: In fracture pattern AO/OTA 31-A2, PFN without distal interlocking had better results and less complications than PFN with distal interlocking.
Keywords: Arbeitsgemeinschaft für Osteosynthesefra-gen/Orthopaedic Trauma Association 31-A1 and 31-A2; Distal interlocking screws; Intertrochanteric fracture; Outcome; Proximal femoral nail; Without distal interlocking screws.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they do not have any conflicts of interest.
Figures



Similar articles
-
Short versus long proximal femoral nail in the management of intertrochanteric fractures - a comparative study.Int J Burns Trauma. 2023 Jun 15;13(3):99-109. eCollection 2023. Int J Burns Trauma. 2023. PMID: 37455801 Free PMC article.
-
The treatment of reverse obliquity intertrochanteric fractures with the intramedullary hip nail.J Trauma. 2008 Oct;65(4):852-7. doi: 10.1097/TA.0b013e31802b9559. J Trauma. 2008. PMID: 18849802
-
Parameters Governing the Fate of Fracture Fixation With Proximal Femoral Nailing (PFN) for Intertrochanteric Femur Fractures.Cureus. 2023 Jun 25;15(6):e40952. doi: 10.7759/cureus.40952. eCollection 2023 Jun. Cureus. 2023. PMID: 37503460 Free PMC article.
-
Proximal femoral nailing is superior to hemiarthroplasty in AO/OTA A2 and A3 intertrochanteric femur fractures in the elderly: a systematic literature review and meta-analysis.Int Orthop. 2020 Apr;44(4):623-633. doi: 10.1007/s00264-019-04351-9. Epub 2019 Jun 14. Int Orthop. 2020. PMID: 31201487
-
[Progress on distal interlocking screw of cephalomedullary nail for intertrochanteric fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014 Sep;28(9):1177-80. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014. PMID: 25509788 Review. Chinese.
Cited by
-
[Research progress on distal interlocking screws of cephalomedullary nails in intertrochanteric fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Mar 15;38(3):356-362. doi: 10.7507/1002-1892.202312052. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 38500431 Free PMC article. Chinese.
-
Effect of proximal femoral nail antirotation on clinical outcome, inflammatory factors and myocardial injury markers in patients with femoral trochanteric fracture.Am J Transl Res. 2022 Jul 15;14(7):4795-4803. eCollection 2022. Am J Transl Res. 2022. PMID: 35958501 Free PMC article.
References
-
- Kregor PJ, Obremskey WT, Kreder HJ, Swiontkowski MF Evidence-Based Orthopaedic Trauma Working Group. Unstable pertrochanteric femoral fractures. J Orthop Trauma. 2005;19:63–66. - PubMed
-
- Schipper IB, Steyerberg EW, Castelein RM, van der Heijden FH, den Hoed PT, Kerver AJ, van Vugt AB. Treatment of unstable trochanteric fractures. Randomised comparison of the gamma nail and the proximal femoral nail. J Bone Joint Surg Br. 2004;86:86–94. - PubMed
-
- Boldin C, Seibert FJ, Fankhauser F, Peicha G, Grechenig W, Szyszkowitz R. The proximal femoral nail (PFN)--a minimal invasive treatment of unstable proximal femoral fractures: a prospective study of 55 patients with a follow-up of 15 months. Acta Orthop Scand. 2003;74:53–58. - PubMed
LinkOut - more resources
Full Text Sources
