

Diagnosis, treatment and complications of radial head and neck fractures in the pediatric patient
- PMID: 35317255
- PMCID: PMC8935328
- DOI: 10.5312/wjo.v13.i3.238
Diagnosis, treatment and complications of radial head and neck fractures in the pediatric patient
Abstract
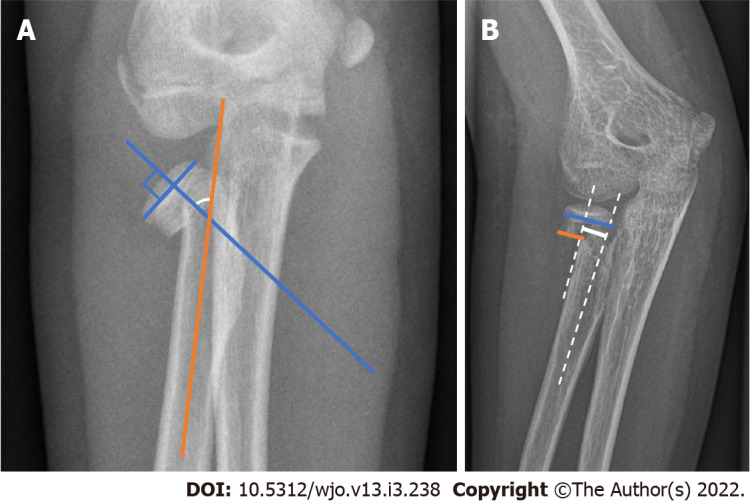
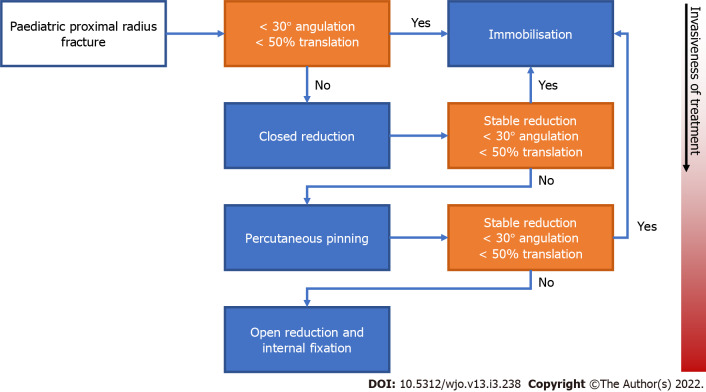
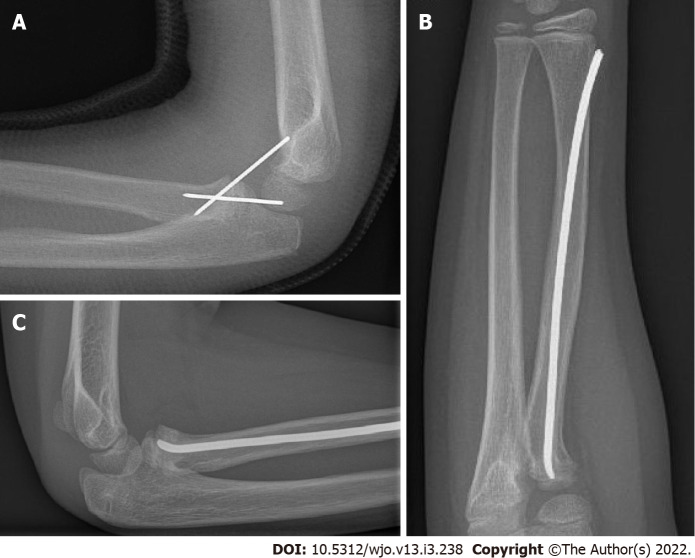
Radial head and neck fractures represent up to 14% of all pediatric elbow fractures and can be a difficult challenge in the pediatric patient. In up to 39% of proximal radius fractures, there is a concomitant fracture, which can easily be overlooked on the initial standard radiographs. The treatment options for proximal radius fractures in children range from non-surgical treatment, such as immobilization alone and closed reduction followed by immobilization, to more invasive options, including closed reduction with percutaneous pinning and open reduction with internal fixation. The choice of treatment depends on the degree of angulation and displacement of the fracture and the age of the patient; an angulation of less than 30 degrees and translation of less than 50% is generally accepted, whereas a higher degree of displacement is considered an indication for surgical intervention. Fractures with limited displacement and non-surgical treatment generally result in superior outcomes in terms of patient-reported outcome measures, range of motion and complications compared to severely displaced fractures requiring surgical intervention. With proper management, good to excellent results are achieved in most cases, and long-term sequelae are rare. However, severe complications do occur, including radio-ulnar synostosis, osteonecrosis, rotational impairment, and premature physeal closure with a malformation of the radial head as a result, especially after more invasive procedures. Adequate follow-up is therefore warranted.
Keywords: Closed fracture reduction; Fracture; Fracture fixation; Open reduction fracture; Osteonecrosis; Pediatrics; Proximal radius; Radial head; Synostosis.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare no conflict of interest for this article.
Figures


References
-
- Radomisli TE, Rosen AL. Controversies regarding radial neck fractures in children. Clin Orthop Relat Res. 1998:30–39. - PubMed
-
- Nicholson LT, Skaggs DL. Proximal Radius Fractures in Children. J Am Acad Orthop Surg. 2019;27:e876–e886. - PubMed
-
- Landin LA. Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950-1979. Acta Orthop Scand Suppl. 1983;202:1–109. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
