

Role and Extent of Neck Dissection for Neck Lymph Node Metastases in Differentiated Thyroid Cancers
- PMID: 35317376
- PMCID: PMC8907697
- DOI: 10.14744/SEMB.2021.76836
Role and Extent of Neck Dissection for Neck Lymph Node Metastases in Differentiated Thyroid Cancers
Abstract
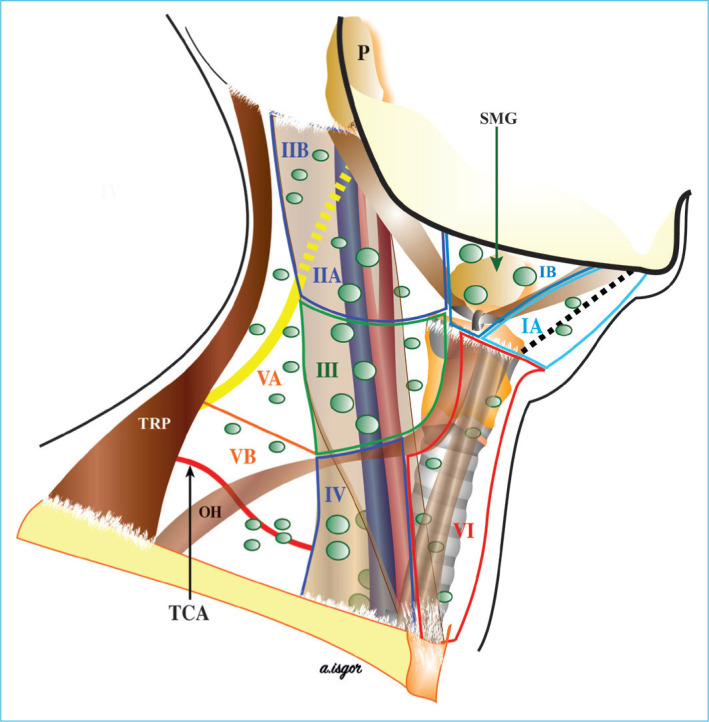
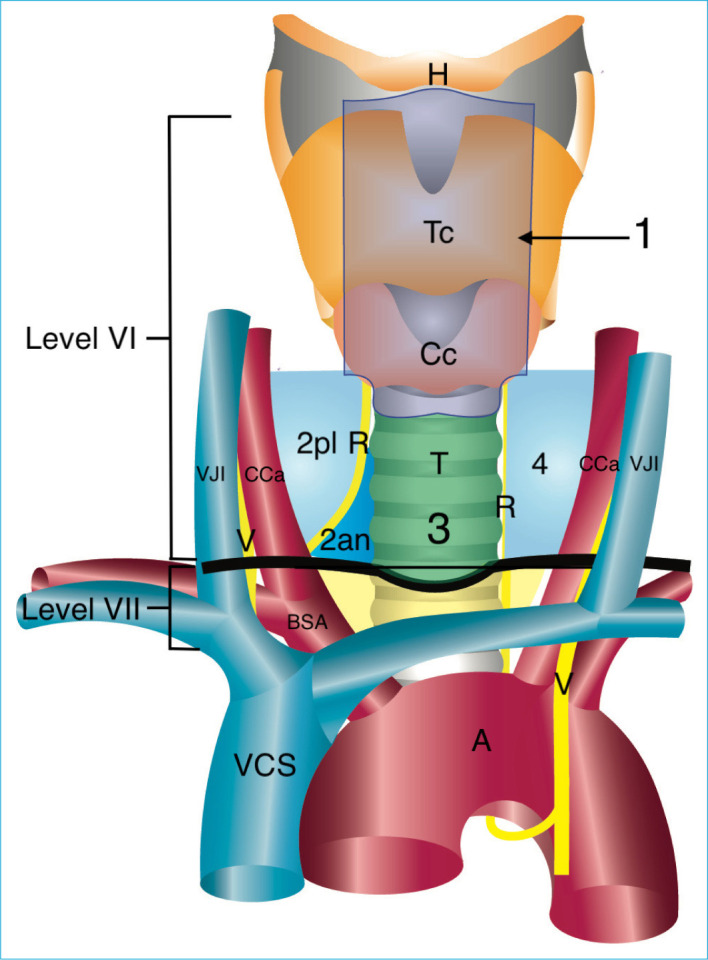
Differentiated thyroid cancers (DTC) consist of 95% of thyroid tumors and include papillary thyroid cancer (PTC), follicular thyroid cancer (FTC), and Hurthle cell thyroid cancer (HTC). Rates of lymph node metastases are different depending on histologic subtypes and <5% in FTC and between 5% and 13% in HTC. Lymph node metastasis is more frequent in PTC and while rate of clinical metastasis can be seen approximately 30% rate of routine micrometastasis can be seen up to 80%. Lymph node metastasis of DTC mostly develops first in the Level VI lymph nodes at the central compartment starting from the ipsilateral paratracheal lymph nodes and then spreading to the contralateral paratracheal lymph nodes. Spread to the Level VII is mostly after Level VI invasion. Subsequent spread is to the lateral neck compartments of Levels IV, III, IIA, and VB and sometimes to the Levels IIB and VA. Occasionally skip metastasis to the lateral neck compartments develop without spreading to the central compartments and this situation is more frequent in upper pole tumors. Although application of prophylactic central neck dissection (pCND) in DTC increases the rate of complication, due to its unclear effects on oncologic results and quality of life, the interest to the pCND is decreasing and debate on its surgical extent is increasing. pCND is not essential in DTC and characteristics of patient and tumor and experience of surgeon should be considered when deciding for pCND. Due to lower complication rate of one sided pCND compared to bilateral central neck dissection (CND), low possibility of contralateral central neck metastasis and low risk of recurrence, application of one-sided CND is logical. Although therapeutic CND (tCND) is the standart treatment when there is a clinically involved lymph node, extent of dissection is a matter of debate. A case-based decision for the extent of tCND can be made by considering patient and tumor characteristics and experience of the surgeon. Due to the higher complication risk of bilateral CND, unilateral tCND can be performed if there is no suspicious lymph node on the contralateral side and bilateral tCND can be applied when there is a suspicion for metastasis only on the contralateral side or there are features for risk of metastasis to the contralateral side. In patients with clinical central metastasis owing to intra-operative pathology results by frozen section procedure are compatible with post-operative pathology results, when there is a suspicion for contralateral metastasis, a decision for one- or two-sided dissection can be made using frozen section procedure. In DTC, it can be stated that there is a consensus in the literature about not performing prophylactic lateral neck dissection (LND), but performing therapeutic LND (tLND). In addition, there is a debate on the extent of tLND. In a meta-analysis about lateral metastasis, the rates of metastasis to the Levels IIA, IIB, III, IV, VA, and VB were 53.1%, 15.5%, 70.5%, 66.3%, 7.9%, and 21.5%, respectively. Ultrasonography (USG) is an effective procedure for detection of cervical nodal metastasis on lateral compartment. Pre-operative imaging with USG and/or combination with the fine needle aspiration biopsy (cytology/molecular test/Thyroglobulin test) can allow pre-operative detection and verification of lateral lymph node metastasis. Extent of tLND can be determined to minimize morbidity considering pre-operative USG findings, pre-operative tumor and clinical features of lateral metastasis. Especially in the presence of limited lateral metastases, limited selective LND such as Levels III, IV or Levels IIA, III, IV can be applied according to the patient. Levels IIB and VB should be added to the dissection in the presence of metastases in these regions. In cases that increase the risk of Level IIB involvement, such as presence of metastasis at Level IIA, extranodal tumor involvement, presence of multifocal tumor, and in cases that increase the risk of Level VB involvement such as macroscopic extranodal spread, and simultaneous metastases at Levels II, III, IV; Levels IIB and VB can be added to dissection material. Levels I and VA should be added to the dissection in the presence of clinically detected metastases.
Keywords: Differentiated thyroid cancers; Lymph nodes; Metastasis; Neck dissection.
Copyright © by The Medical Bulletin of Sisli Etfal Hospital.
Figures
References
-
- Wiltshire JJ, Drake TM, Uttley L, Balasubramanian SP. Systematic review of trends in the incidence rates of thyroid cancer. Thyroid. 2016;26:1541–52. - PubMed
-
- Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Kosary CL, et al. National Cancer Institute; 2017. SEER Cancer Statistics Review 1975–2014 National Cancer Institute SEER Cancer Statistics Review 1975–2014; pp. 2012–2014.
-
- Vriens MR, Suh I, Moses W, Kebebew E. Clinical features and genetic predisposition to hereditary nonmedullary thyroid cancer. Thyroid. 2009;19:1343–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources